

Zachary A. Weber, PharmD, BCPS, BCACP, CDE
- Clinical Associate Professor, Department of Pharmacy Practice, Purdue University College of Pharmacy, Indianapolis, Indiana

https://www.pharmacy.purdue.edu/directory/zaweber
There may be supine hypertension and reversal of the normal circadian blood pressure rhythm (normally lower at night) mood disorder ppt best 25 mg amitriptyline, with an increased frequency of micturition at night depression paranoia buy discount amitriptyline 25mg on line. Other features of autonomic dysfunction may be present depression symptoms shaking effective amitriptyline 50mg, including dry eyes and dry mouth (xerophthalmia anxiety back pain order amitriptyline 25mg line, xerostomia) anxiety quiz online discount 50mg amitriptyline fast delivery, a tendency to constipation depression dsm buy amitriptyline without prescription, and lack of penile erections. Guillain–Barré syndrome, amyloidosis) However, the most common cause of orthostatic hypotension in hospital practice is probably dehydration or overzealous treatment with antihypertensive or diuretic agents. Management of orthostatic hypotension consists of education on fac tors that influence blood pressure. Non-pharmacological approaches include increased salt and water intake, head-up bed tilt, and wearing elastic stockings or a G-suit. Pharmacological therapies include fludrocortisone (first line), and midodrine, ephedrine, or dihydroxyphenylserine (second line). Cross References Neuropathy; Parkinsonism; Xerophthalmia, Xerostomia -257 O Oscillopsia Oscillopsia Oscillopsia is an illusory movement of the environment due to excessive slip of images on the retina (‘retinal slip’) during active or passive head movement, producing a complaint of blurring, jumping, or oscillation of the visual repre sentation of the environment. Oscillopsia is most often due to acquired bilateral loss of vestibular function (loss of the vestibulo-ocular reflexes). Oscillopsia does not occur in congenital nystagmus, nor in opsoclonus, presumably due to the operation of the visual suppression mechanism which normally operates during saccadic eye movements. Oscillopsia: impaired vision during motion in the absence of the vestibulo-ocular reflex. Cross References Myokymia; Nystagmus; Opsoclonus; Vestibulo-ocular reflexes Oscillucusis Oscillucusis is an abnormal perception of an oscillation in the intensity of ambient sounds, which may occur during a migraine attack. Osmophobia Osmophobia, an aversion to smells, may form part of a migraine attack, along with photophobia and phonophobia. A distinction may be made between essential and symptomatic palatal tremor, also known as primary and secondary isolated palatal tremor. Palatal tremor may be asymptomatic or there may be a clicking sound in the inner ear, especially in essential palatal tremor. There may be associated contractions of external ocular muscles (oculopalatal myoclonus), larynx, neck, diaphragm (respiratory myoclonus, diaphragmatic flutter, or Leeuwenhoek’s dis ease), trunk, and limbs, which may bring the palatal tremor to attention. Palatal myoclonus is associated with lesions interrupting pathways between the red nucleus, inferior olivary nucleus, and dentate nucleus (Guillain–Mollaret triangle). Hypertrophy of the inferior olivary nucleus may be evident neuro radiologically (structural or functional imaging) and pathologically. This is a consequence of a lesion in the dentato-olivary pathway which leads to transsy naptic degeneration and hypermetabolism of the olivary nucleus. Although many cases are essential/idiopathic, recognized symptomatic causes of palatal tremor include vascular lesions, trauma, neoplasia, demyelination, epilepsy, and, rarely, adult-onset Alexander’s disease. Drug treatment of palatal tremor is often unsuccessful, although reports of benefit with 5-hydroxytryptophan, carbamazepine, sodium valproate, clon azepam, baclofen, and even sumatriptan have appeared. Cross References Eight-and-a-half syndrome; Myoclonus; Nystagmus; Oscillopsia; Tinnitus; Tremor Palilalia Palilalia is a disorder of articulation characterized by the involuntary repetition of syllables within a word, whole words, or phrases, hence a reiterative speech A. The term stutter may be used for repetition of single syllables, and the term palilogia has sometimes been used for the repetition of phrases, to distinguish from palilalia. Although sometimes classified as an illusory experience, musical hallucinations may occur concurrently. Cross References Hallucination; Illusion Palinopsia Palinopsia is an illusory visual phenomenon characterized by the persistence or recurrence of visual images immediately after the stimulus has been removed, hence visual perseveration. The description of the symptom may lead to it being mistaken for diplopia (‘pseudodiplopia’). Palinopsia occurs most frequently in the context of a left homonymous hemi anopia, secondary to right occipitotemporal or occipitoparietal lesions: these may be vascular, neoplastic, metabolic, ictal, or drug or toxin-induced. It has also been described with retinal and optic nerve disease and occasionally in normal individuals. Object-specific and “side inversed” palinopsia limited to the hemianopic field in occipital infarction. Cross References Hemianopia; Illusion; Perseveration; Polyopia; Visual perseveration Pallaesthesia Pallaesthesia is the appreciation of vibration sensation; its loss may be described as pallanaethesia. Cross Reference Vibration Palmaris Brevis Sign Palmaris brevis sign may be useful in localizing the site of an ulnar nerve lesion. Innervated by the superficial ‘sensory’ division of the ulnar nerve in the wrist (distal canal of Guyon), contraction of the palmaris brevis muscle may be evi dent with compressive lesions of the deep motor branch of the ulnar nerve which cause intrinsic hand muscle weakness but no sensory loss (‘Ramsay Hunt syn drome’): ask the patient to ‘contract’ the hypothenar eminence with the fifth digit forcibly abducted and look for skin corrugation. Palmomental Reflex the palmomental reflex consists of contraction of the mentalis muscle induced by stroking the ipsilateral palm with a blunt object. It may indicate damage to the contralateral paracentral cortex or its connections, but since it is observed in about one quarter of normal adults and is very common in the normal elderly, and may occur in other conditions, both its sensitivity and specificity are low. It may be considered a frontal release sign or primitive reflex, but is less specific than the grasp reflex. Induction of the reflex by stimulation of areas other than the palm is more likely to be associated with cerebral damage. Cross References Age-related signs; Frontal release signs Pandysautonomia Pandysautonomia is characterized by pre and postganglionic lesions of both the sympathetic and parasympathetic pathways. Papilloedema Papilloedema is swelling (oedema) of the optic nerve head due to raised intracra nial pressure (cf. A number of stages of papilloedema are described: in the acute stage, the only findings may be oedema at the superior and inferior poles of the disc, absence of spontaneous venous pulsation, and enlargement of the blind spot. As papilloedema progresses the whole disc is involved and splinter haemorrhages may be evident at the disc margin. These early stages may be asymptomatic or may be associated with transient losses of vision (obscurations), often pro voked by activities or movements which further raise intracranial pressure, thus compromising retinal perfusion pressure. Enlargement of the blind spot and con striction of the visual field may be evident, but visual acuity is often unimpaired (cf. Chronic papilloedema produces gliosis of the optic nerve head and eventually optic atrophy (‘sequential optic atrophy’) with nerve fibre damage and permanent visual field defects. Guillain–Barré syndrome, acid maltase deficiency, phrenic nerve injury, hence paradoxical abdominal movement, abdominal paradox, paradox ical breathing, or paradoxical diaphragm movement. Paradoxical diaphragm movement is a potentially alarming sign since it may indicate incipient respiratory failure. The term paradoxical breathing may also be used to describe thorax and abdomen moving in different directions when breathing, as with increased upper airway resistance. Some patients may describe this sensation as ‘numb ness’ or ‘deadness’, in which case care needs to be taken to differentiate it from anaesthesia. Some authorities reserve the term for spontaneous rather than evoked positive sensory phenomena, as a distinction from dysaesthesia. Paraesthesia is a feature of neuropathy and may occur in the distribution of a compressed or entrapped nerve, perhaps reflecting the mechanosensitivity of nerves in this situation. Paraesthesia is a more reliable indicator of the diagnosis of neuropathy than pain. Paraesthesia may also be provoked by hyperventilation (especially perioral, hands, and feet [acroparaes thesia]). Missed diagnosis of vitamin B12 deficiency presenting with paraes thetic symptoms. Cross References Anaesthesia; Dysaesthesia; Lhermitte’s sign; Phalen’s sign; Tinel’s sign -263 P Paragrammatism Paragrammatism Paragrammatism is the substitution of morphological elements and function words in the context of fluent speech. Wernicke’s aphasia), as differentiated from agrammatism, the omission of function words and bound morphemes in non-fluent speech. It should be remem bered that many movements previously thought to conform to this definition have subsequently been recognized to have an organic basis. The use of the word has not been entirely consistent, for example, paral ysis agitans originally used by James Parkinson to describe the disease which now bears his name. The periodic paralyses are a group of conditions characterized by episodic muscular weakness and stiffness (myotonia) associated with muta tions in the skeletal muscle voltage-gated sodium and calcium ion channel genes (channelopathies). Cross References Myotonia; Plegia Paramnesia Paramnesia is recalling as memories things which have not in fact taken place, hence a distortion of episodic or autobiographical memory. Cross References Amnesia; Confabulation; Reduplicative paramnesia 264 Paraparesis P Paramyotonia Paramyotonia is similar to myotonia in that muscle does not relax normally fol lowing contraction (voluntary, percussion), which may prompt a complaint of muscle aching or stiffness, but differs in that repetitive muscle use. For example, repeated forced voluntary eyelid closure in a patient with paramyotonia may, after several attempts, lead to a failure of volun tary eyelid opening, the eyes remaining closed for a minute or so. This type of muscle stiffness may also be sensitive to temperature, being made worse by cooling which may also provoke muscle weakness. During the delayed muscle relaxation, electrical activity is not prominent, and after muscle cooling the resting muscle membrane potential may be reduced from around the normal −80 to −40 mV, at which point muscle fibres are inexcitable (contracture). Mutations in the same gene have been documented in hyperkalaemic periodic paralysis and K+-aggravated myotonia. Symptomatic treatment with membrane-stabilizing agents like mexiletine and tocainide or with the carbonic anhydrase inhibitor acetazolamide might be tried. Precautions are necessary during general anaesthesia because of the risk of diaphragm myotonia. Paramyotonia congenita and hyper kalaemic periodic paralysis are linked to the adult muscle sodium channel gene. Cross References Contracture; Myotonia; Paralysis; Warm-up phenomenon Paraparesis Paraparesis is a weakness of the lower limbs, short of complete weakness (para plegia). This may result from lesions anywhere from cerebral cortex (frontal, parasagittal lesions) to peripheral nerves, producing either an upper motor neu rone (spastic) or lower motor neurone (flaccid) picture. Upper motor neurone lesions: Traumatic section of the cord; Cord compression from intrinsic or extrinsic mass lesion. Cross References Flaccidity; Myelopathy; Paraplegia; Spasticity Paraphasia Paraphasias are a feature of aphasias (disorders of language), particularly (but not exclusively) fluent aphasias resulting from posterior dominant temporal lobe lesions (cf. Paraphasias refer to a range of speech output errors, both phono logical and lexical, including substitution, addition, duplication, omission, and transposition of linguistic units, affecting letters within words, letters within syllables, or words within sentences. Phonemic paraphasias may be encountered in Broca’s aphasia and conduction aphasia, when the patient may recognize them to be errors, and Wernicke’s aphasia. These may be further classified as: Semantic or categoric: substitution of a different exemplar from the same category. Verbal paraphasias showing both semantic and phonemic resemblance to the target word are called mixed errors. These types may be observed in patients with Wernicke’s aphasia, who often seem unaware of their paraphasias due to a failure of self-monitoring of output. This may result from lower motor neurone lesions involving multiple nerve roots and/or peripheral nerves. The latter may acutely produce a flaccid areflexic picture (‘spinal shock’), but later this develops into an upper motor neurone syndrome (hypertonia, clonus, hyperreflexia, loss of superficial reflexes [e. In paraplegia of upper motor neurone origin, enhanced flexion defence reflexes (‘flexor spasms’) may occur, producing hip and knee flexion, ankle and toe dorsiflexion. Eventually such flexor responses may become a fixed flexion deformity with secondary contractures (‘paraplegia in flexion’). Prevention of this situation may be possible by avoiding spasms, which are often provoked by skin irritation or ulceration, bowel constipation, bladder infection, and poor nutrition. Physiotherapy and pharmacotherapy with agents such as baclofen, dantrolene, and tizanidine may be used; botulinum toxin injections may be help ful for focal spasticity. Since localized pain may inhibit voluntary muscular exertion, apparent weakness in such circumstances may be labelled ‘algesic pseudoparesis’. The key anatomical substrates, damage to which causes the syndrome, are probably the intersti tial nucleus of Cajal and the nucleus of the posterior commissure and their projections. Cross References Collier’s sign; Light-near pupillary dissociation; Nystagmus; Supranuclear gaze palsy Parkinsonism Parkinsonism is a clinical syndrome characterized by the presence of some or all of the following features; there is overlap with so-called akinetic-rigid syndromes in which these features predominate: Insight into the non-reality of these experiences may be retained, hence ‘pseudohallucinations’. Autonomic dysfunction, especially orthostatic hypotension Conventionally parkinsonism is viewed as a disorder of the extrapyrami dal system producing ‘extrapyramidal signs’, although this term has limitations: despite the fact that some of the cardinal features of parkinsonism (bradykinesia, rigidity, postural instability, tremor) result from pathology in the basal ganglia, particularly affecting dopaminergic pathways, other features may reflect cortical involvement, at least in part. The incidence of parkinsonism increases dramatically with age; it is also associated with an increased risk of death, particularly in the presence of a gait disturbance. It is crucial not to miss the diagnosis of Wilson’s disease, although rare, since in the early stages this disorder is reversible with copper chelation therapy; hence copper and caeruloplasmin should be checked in all patients with young-onset (under age 50) parkinsonism (and dystonia). Response to levodopa therapy is only reliably seen in idiopathic Parkinson’s disease, although some patients with multiple system atrophy or progres sive supranuclear palsy may benefit. The features particularly responsive in Parkinson’s disease are bradykinesia and rigidity; tremor is less reliably helped. Prevalence of parkinsonian signs and associated mortality in a community population of older people. Cross References Apraxia; Blinking; Bradykinesia; Dysarthria; Dystonia; Hypokinesia; Hypomimia; Hypophonia; Mask-like facies; Micrographia; Orthostatic hypotension; Postural reflexes; Rigidity; Seborrhoea; Sialorrhoea; Striatal toe; Supranuclear gaze palsy; Tremor Parosmia Parosmia is a false smell, i. Such smells are usually unpleasant (cacosmia), may be associated with a disagreeable taste (cacogeusia), and may be difficult for the patient to define. Causes include purulent nasal infections or sinusitis and partial recovery following transection of olfactory nerve fibres after head injury. Transient parosmia may presage epileptic seizures of temporal lobe corti cal origin (olfactory aura), particularly involving the medial (uncal) region. Cross References Aura; Seizures Parry–Romberg Syndrome Hemifacial atrophy is thinning of subcutaneous tissues on one side of the face; it may also involve muscle and bone (causing enophthalmos), and sometimes brain, in which case neurological features (hemiparesis, hemianopia, focal epileptic seizures, cognitive impairment) may also be present. The clinical heterogeneity of hemifacial atrophy probably reflects patho genetic heterogeneity. The syndrome may result from maldevelopment of auto nomic innervation or vascular supply, or as an acquired feature following trauma, or a consequence of linear scleroderma (morphoea), in which case a coup de sabre may be seen. Some observations on the aetiology of hemifacial atrophy (“Parry–Romberg syndrome”). There may be a sense that the patient is strug gling against these displays of emotion, in contrast to the situation in other forms of emotional lability where there is said to be congruence of mood and affect, although sudden fluctuations and exaggerated emotional expression are common to both, suggesting a degree of overlap. Pathological laughter and crying following stroke: validation of a measurement scale and a double-blind treatment study. Cross References Automatism; Emotionalism, Emotional lability; Pseudobulbar palsy Peduncular Hallucinosis Peduncular hallucinosis is a rare syndrome characterized by hallucinations and brainstem symptoms. Brainstem find ings include oculomotor disturbances, dysarthria, ataxia, and impaired arousal.
Rupture of the epigastric vessels leads to accumulation of large collection of blood in the front abdominal Vieira C depression glass test order amitriptyline online. She was hypotensive 70/50mmHg mood disorder questionnaire-adolescent order 25mg amitriptyline otc, tachycardic 130/ 3 min anxiety zone generic 25mg amitriptyline with amex, anuric depression symptoms online test purchase amitriptyline canada, anxious and confused anxiety 2 days after drinking buy amitriptyline american express. She was preoperatively stabilized by colloids severe depression vs bipolar order line amitriptyline, crystalloids characterized by blistering and epithelial sloughing. The incidence the surgery two liters of coagulum was evacuated and ligation of the artery was is approximately one to two cases per million per year. She was extubated after few hours and transferred to the ward acute illness often develop signifcant long-term sequelae. A p value inferior to 0,05 was considered include Hemophilia and Von Willebrand disease and overdose with anticoagulants. Masanori Shimodaira et al: An oblique muscle hematoma as a rare cause of and 13% overlap syndrome. In 37% of Learning points: Hematomas in the abdominal wall can often mimic various patients the aetiology agent stayed uncertain. All of them went to conservative treatment measures, 17% to plasmapheresis and 20% to surgical cleaning. One case of A case of Fournier’s Gangrene in a 52 years old female disseminated intravascular coagulation occurred. Our series showed an overall in hospital mortality of 47%, which was higher than the expected mortality based on Nella A. She showed an ulcerated gluteus abscess with eschar from right inguinal region to half thigh wide. Metamizole different factors, such as nutrition, immunological response and genetic factors. Chest causative agent may be straightforward as in here where a single drug is implicated, scan showed pleural effusion and infltration on both sides. Surgery was performed but diffculties are posed when the patient has been exposed to multiple drugs. All patients should pyelonephritis at right side, hepatosplenomegalia, signs of periportal oedema and be submitted to blood analysis, chest x-ray, tissue biopsy, swabs from lesional skin distension of intestines. Skin management may involve a conservative and/or surgical procedure: Relaparatomia mediana superior et inferior, Nephrectomio l. Hormone of thyreoid a conservative approach, based on the specialist multi-disciplinary team’s daily glandulae was done and showed Hypothyroidism subclinical. Journal of Plastic, Reconstructive & correction of appropriate therapy and introduction of gluten-free food. These fndings may infuence clinical agent, and specialized supportive care, ideally in an intensive care unit, in order to management and primary prevention of kidney diseases in patients with celiac achieve the best outcome for these patients. In the majority of causes the condition may be clinically silent and found only by active case-fnding in celiac disease risk groups. The early diagnosis of sepsis and the establishment of appropriate and timely treatment may both considerably improve the outcome. The epidemiology of candidemia actually an inadequate tissue perfusion, with a multiple possible ethiologies and is changing with an increase in the proportion of Candida (C. There can be all the possible reasons, separately or even co-exist from Materials and Methods: A retrospective review of consecutive adult surgical losing blood, particularities of neurologic injuries, hypoxemia, obstructive forms, patients with candidemia between June 1, 2014 and April 30, 2016, was conducted. Results and Discussion: During this period, a total of 20 cases of Candidemia Case Report: this is a case of a 67 years old female patient, with a multiple were identifed; 8 women (44%) and 12 men (56%), with a mean age of 75 years trauma, victim of a car accident (pedestrian), with complex traumatic lesions – (range 68-83). The life support was immediately started, concomitant with the (55%), followed by C. After identifcation of complex and invasive monitoring for the diagnosis of the shock – specifc invasive the causative species and susceptibility testing results, treatment was modifed hemodynamic monitoring (transpulmonary thermodilution and transesophageal in 4 patients (20%). Overall mortality was 45%, and 3 (30%) of 9 deaths occurred echocardiography), thromboelastometry and serial imagistic exams within 48 hours of the detection of candidemia. Initially, the rapidly fatal underlying illness, and sustained positivity of blood cultures. After 24h, there is an improvement -Non-albicans Candida species reach almost half of the Candida isolates in the hemodynamic status, clinical signs and lab results. This response to the -An early fatal outcome promoted by candidemia may be prevented with empirical treatment was a statement for the diagnosis of neurogenic shock. The aim of this study was to evaluate of Medicine and Pharmacy Craiova (Romania), Department of the the effcacy of anidulafungin for the treatment of candidaemia and invasive Clinical Pharmacology, University of Medicine and Pharmacy Craiova candidiasis in high risk surgical patients. Preventive anidulafungin therapy was given until resolution of the which affect the whole body. The most common baseline Candida species were Candida albicans (aggravated chronic hepatitis, decompensated liver cirrhosis, hepatic encefalopaty, (56%), C. In 15% of the Materials and Methods: this retrospective study included 113 hepatic patients isolates, the causative Candida was less susceptible or resistant to fuconazole. However, Clinical Emergency Hospital of Craiova, Romania for hidric re-equilibration and it was 44 % in patients with candidemia and 80% in patients with Candida Krusei. We extracted from patients’ electronic records the demographic, Conclusions: Non-albicans Candida species reach almost half of the Candida clinical and laboratory data. The risk remains high and adequate antifungal therapy is necessary to lead a goof outcome. This is not surprising as cirrhotic patients have an increased risk for bacterial infections. We isolated from ascitic fuid: Escherichia coli, Klebsiella, Proteus, Enterococcus, Acinetobacter, Methicillin Resistant Staphylococcus aureus and Streptococcus. Although Clinical Pulmonary Infection Score has been used Background: Pneumocystis jirovecii(known as Pneumocystis carinii) is an successfully in medical and surgical patients, the systemic infammation in this important opportunistic fungal pathogen in humans who have depressed immune population limits its utility. The most common isolated bacteria were Pseudomonas aeruginosa (n=6, patient received trimethoprim (20 mg/kg per days)sulfamethoxazole for 7 days 31,6%) and Klebsiella pneumoniae (n=6, 31,6%). Acute circulatory failure the patient demanded included Methicillin-susceptible Staphylococcus aureus, Enterococcus faecium, continuous infusion of vasopressive agents. Prone position was applied four Enterobacter cloacae, Acinetobacter baumannii and Serratia marcescens. The diagnosis was based on tuberculosis, and fungi, should be considered in all rheumatological patients on invasive cultures but the true incidence of burn respiratory infections remains to treatment who present to intensive care. Microcirculation damage and endothelial dysfunction have already been described in sepsis, but their involvement in coronary circulation still needs to be investigated. The present study aimed to assess microcirculatory and endothelial vasomotor function in an experimental model of faecal peritonitis sepsis in pigs. After anaesthesia induction, a pressure/fow wire (Volcano ComboWire) was placed in the mid-portion of the left anterior descending coronary artery under. Stimulation of angiotensin type 2 receptor attenuates Hyperaemia was obtained by intracoronary bolus of 3 mL adenosine (90 µg) and 3 mL bradykinin (10-6M) to test respectively the microcirculatory endothelium organ injury in rats with polymicrobial sepsis. However, data on regulative properties of this receptor on the sepsis response are poor. Then we measure the arterial blood pressure, heart rate, and organ function index of lung, (Ukraine), 2Kyiv Hepatobiliary and Pancreatic Surgery Center Kyiv liver and kidney. During the entire period of treatment, 178 crops were performed for all patients (drainages n=98, urine n=42, tracheal aspirates n=38); which were repeated every 3-4 days for the purpose of control agent and antibiotics sensitivity. Conclusions: Resistance to antimicrobial drugs jeopardizes effective prevention and treatment of a growing range of bacterial infections. As practice shows, to achieve Background and Goal of Study: the enormous morbidity associated with sepsis adequate blood pressure and tissue perfusion in patients with refractory septic and consequent organ failure necessitates resuscitation and treatment at the shock, it is not enough just to infuse crystalloids and vasoactive drugs. Equally important, is the prediction of outcome at admission in order to in recent years, the use of terlipressin has become a very promising treatment for differentiate patients with more severe disease and direct therapies accordingly. Emerging necrosis of ascending Materials and Methods: In this observational prospective study, 130 adult colon. The administration of terlipressin binary regression linear model, these variables were evaluated as markers for day and hydrocortisone was discontinued 24 hours after the start, positive dynamics 28 mortality. On the 7th day, the patient was transferred to the surgical department for some of the variables under study were signifcantly different (p <0. Thrombocytopenia in sepsis, which occurs since catecholamines have a detrimental effect on the immune function, they due to multiple immune and non-immune mechanism, underlines deterioration of stimulate bacterial growth, and cause myocardial damage. But at the same time, the use of biomarkers to help identify patients with a high risk of mortality is appealing. A sequential organization failure all-cause mortality in adult patients with sepsis. Recent studies have revealed that the trajectory from baseline studies of adult patients with sepsis, any randomized trials were excluded. Student’s t concentration (non-survivors – survivors), measured at onset of sepsis, are listed test or Mann-Whitney tests were used to compare continuous variables, Pearson as follows: chi-square test was used to compare categorical variable. The hemodynamic and volumetric variables, blood gases and biochemical parameters were measured at all three stages of the study. In the present study, we investigated the effects of dexmedetomidine Bermejo-Martín J. Patients were randomly 3Anesthesiology and Reanimation Service, Hospital Universitario divided into Dexmedetomidine group (group D, n=25) and control group (group Río Hortega Valladolid (Spain), 4Anesthesiology and Reanimation C, n=25). In group D, patients received a loading infusion of Dexmedetomidine (1μg•kg) intravenously for 20min before induction of anesthesia and followed by-1 Service, Complejo Asistencial Universitario Salamanca Salamanca -1 (Spain), 5Department of General and Gastrointestinal Surgery, Complejo a maintenance infusion [0. In group C, the patients received matching placebo (equal volume of normal saline). Sepsis represents the major cause of death among critically ill were signifcantly increased in the two groups at T2 and T3, but the increase was patients, constituting an important public health problem. The infuence of infusion therapy of different Learning points: Cardiac abnormalities suggestive for stress cardiomyopathy composition on the dynamics of cerebral circulation are rare but important fndings in patients presenting with intracranial hemorhage. Doctors should be aware of this complication which can lead to poor treatment and in patients with acute ischemic stroke. Background and Goal of Study: Taking into account the multifaceted nature of 1 1 1 1 the pathogenesis of ischemic damage to the brain, the pharmacological stroke Van Zundert T. The goal of the work was a characteristic guidelines of the brain trauma foundation still advocate the use of barbiturates to of the effect of 0. We identifed a total of 15 brain injured patients with intracranial Evaluation of cerebral hemodynamic was performed using doppler ultrasound of hypertension treated with barbiturates (thiopental). It can also associate with Takotsubo cardiomyopathy, sometimes leading to serious diffculties in diagnostic and treatment management. The patient was perfectly healthy before and she had no signs of trauma or intoxication. The patient had akinesia on all basal segments with hyperkinesia of the apex and an ejection fraction of 25%. After 6 hours of intensive care treatment, brain herniation occurred and the patient was determined to be brain dead. With the family’s approval, the patient’s organs were harvested for transplantation. The usual Takotsubo pattern is apical akinesia and ballooning with basal hiperkinesia. The wall motion pattern in our case report is a rarely described condition named inverted Takotsubo. In our case, the clinical suspicion of acute coronary syndrome was low because of the patient’s presentation and lack of comorbidities. However,9 the preservat ion of a coma and the coming of death in cerebral ischemic stroke patient had frequent seizures, resistant to treatment with levetiracetam, and then is the use of antiplatelet agents. Hyperuricemia most researchers viewed as an thiopental and lacosamide therapy was initiated. On day 30, value of supranormal blood hypoxanthine level in contrast to the hyperuricemia has hemodynamically stable but unconscious patient, breathing spontaneously with been insuffciently studied. There, after a month, the patient died, without any changes control of the blood levels of uric acid and hypoxanthine to predict its course and in clinical status. The importance of other oxypurine by acetyl cholinesterase inhibition – experimental hypoxanthine and xanthine, both in the blood and in the cerebrospinal fuid was study in weanling rats. The purpose of research to compare the value of the level of hypoxanthine, xanthine, uric acid in blood and in the cerebrospinal fuid. Although cortisol blockers in patients with ischemic stroke and hemorrhagic stroke can be used only was the most studied hormone implicated in acute stress, the other endocrine axes if the elevated level of xanthine in the cerebrospinal fuid. This study included eight Wistar rats of the same age, gender and weight the presence of the 1st day elevated level of xanthine in the blood, dihydropyridines that were subjected to chlorpyrifos exposure. They were frst tested for baseline advisable to use in hemorrhagic stroke, regardless of the 1st day elevated levels levels of cholinesterase, cortisol, free triiodothyronine (fT3), thyroxine (fT4), of xanthine in the blood, in ischemic without this. Next samples were taken to determine the level of cholinesterase and with hyperuricemia also not using magnesium sulfate, in hemorrhagic stroke with the above mentioned parameters. Protocol procedures were Conclusion: Among all oxypurines, the level of xanthine in the blood, and not the performed under general anesthesia, according to international guidelines. Levels of cholinesterase were signifcantly decreased after exposure to chlorpyrifos, having a baseline mean value of 1471. Intensive Care Medicine 218 this study demonstrates that besides glucocorticoids, the other axes are also postoperative (n=97, 70. The most frequent site for temperature measurement intoxications, surgery or sepsis, endocrine dysfunctions should be considered. The inadequate sedation could be associated with increasing the high adenoma with intratumorous hemorrhage. Laboratory results reveled hyponatremia risk behaviour such like accidental extubation. On the 19th day after admission transnasal, transphenoidal tumorectomy Nowadays information and communication technology could have a potential to was done. The patient has developed signifcant polyuria resistant on therapy and automate some part of daily practice. Face and body motion data were recorded as video clip by a hydrocortisone 200 mg intravenously for 24 hours (2).
A slow phase with exponentially increasing veloc ity (high-gain instability mood disorder group activities buy 50mg amitriptyline with mastercard, runaway movements) may be seen in congenital or acquired pendular nystagmus depression symptoms worse at night amitriptyline 50 mg with mastercard. The pathophysiology of acquired pendular nys tagmus is thought to be deafferentation of the inferior olive by lesions of the red nucleus depression definition dsm 5 purchase amitriptyline 25mg fast delivery, central tegmental tract depression test lessons4living buy amitriptyline with amex, or medial vestibular nucleus depression unusual symptoms discount amitriptyline 25 mg with mastercard. Nystagmus of peripheral vestibular origin is typically reduced by fixation (hence these patients hold their heads still) and enhanced by removal of visual fixation (in the dark depression test in hindi generic amitriptyline 50mg without prescription, with Frenzel’s lenses). Central vestibular: unidirectional or multidirectional, 1st, 2nd or 3rd degree; typically sustained and persistent. Cerebellar/brainstem: commonly gaze-evoked due to a failure of gaze-holding mechanisms. Congenital: usually horizontal, pendular-type nystagmus; worse with fixation, attention, and anxiety. It may appear with blindness of childhood onset or be acquired with neurological disease (multiple sclerosis, mitochon drial disease, Whipple’s disease, Pelizaeus–Merzbacher disease). Ataxic/dissociated: in abducting >> adducting eye, as in internuclear ophthalmoplegia and pseudointernuclear ophthalmoplegia. Many pathologies may cause nystagmus, the most common being demyelina tion, vascular disease, tumour, neurodegenerative disorders of cerebellum and/or brainstem, metabolic causes. Wernicke–Korsakoff’s syndrome), paraneopla sia, drugs (alcohol, phenytoin, barbiturates, sedative-hypnotic drugs), toxins, and epilepsy. Pendular nystagmus may respond to anticholinesterases, consistent with its being a result of cholinergic dysfunction. Periodic alternating nystagmus responds to baclofen, hence the importance of making this diagnosis. These symp toms are thought to reflect critical compromise of optic nerve head perfusion and are invariably associated with the finding of papilloedema. Obscurations mandate urgent investigation and treatment to prevent permanent visual loss. Cross Reference Papilloedema Obtundation Obtundation is a state of altered consciousness characterized by reduced alert ness and a lessened interest in the environment, sometimes described as psy chomotor retardation or torpor. An increased proportion of time is spent asleep and the patient is drowsy when awake. Cross References Coma; Psychomotor retardation; Stupor Ocular Apraxia Ocular apraxia (ocular motor apraxia) is a disorder of voluntary saccade initia tion; reflexive saccades and spontaneous eye movements are preserved. Ocular apraxia may be overcome by using dynamic head thrusting, with or without blinking (to suppress vestibulo-ocular reflexes): the desired fixation point is achieved through reflex contraversive tonic eye movements to the midposition following the overshoot of the eyes caused by the head thrust. Ocular apraxia may occur as a congenital syndrome (in the horizontal plane only: Cogan’s syndrome), or may be acquired in ataxia telangiectasia (Louis–Bar syndrome), Niemann–Pick disease (mainly vertical plane affected), and Gaucher’s disease (horizontal plane only). Cross References Apraxia; Saccades Ocular Bobbing Ocular bobbing refers to intermittent abnormal vertical eye movements, usu ally conjugate, consisting of a fast downward movement followed by a slow return to the initial horizontal eye position. The sign has no precise localizing value, but is most commonly associated with intrinsic pontine lesions. It has also been described in encephalitis, Creutzfeldt–Jakob disease, and toxic encephalopathies. Its patho physiology is uncertain but may involve mesencephalic and medullary burst neurone centres. Inverse ocular bobbing: slow downward movement, fast return (also known as fast upward ocular bobbing or ocular dipping);. Converse ocular bobbing: slow upward movement, fast down (also known as slow upward ocular bobbing or reverse ocular dipping). Cross Reference Ocular dipping Ocular Dipping Ocular dipping, or inverse ocular bobbing, consists of a slow spontaneous down ward eye movement with a fast return to the midposition. This may be observed in anoxic coma or following prolonged status epilepticus and is thought to be a marker of diffuse, rather than focal, brain damage. Reverse ocular dipping (slow upward ocular bobbing) consists of a slow upward movement followed by a fast return to the midposition. Cross Reference Ocular bobbing Ocular Flutter Ocular flutter is an eye movement disorder characterized by involuntary bursts of back-to-back horizontal saccades without an intersaccadic interval (cf. Ocular flutter associated with a localized lesion in the paramedian pontine reticular formation. It has occasionally been reported with cerebellar lesions and may be under inhibitory cerebellar control. Cross References Hypotropia; Lateral medullary syndrome; Skew deviation; Synkinesia, Synkinesis; Tullio phenomenon; Vestibulo-ocular reflexes Oculocephalic Response Oculocephalic responses are most commonly elicited in unconscious patients; the head is passively rotated in the horizontal or vertical plane (doll’s head maneou vre) and the eye movements are observed. Conjugate eye movement in a direction opposite to that in which the head is turned is indicative of an intact brain stem (intact vestibulo-ocular reflexes). With pontine lesions, the oculocephalic responses may be lost, after roving eye movements but before caloric responses disappear. Cross References Caloric testing; Coma; Doll’s head manoeuvre, Doll’s eye manoeuvre; Head impulse test; Roving eye movements; Supranuclear gaze palsy; Vestibulo-ocular reflexes Oculogyric Crisis Oculogyric crisis is an acute dystonia of the ocular muscles, usually causing upward and lateral displacement of the eye. It is often accompanied by a dis order of attention (obsessive, persistent thoughts), with or without dystonic or dyskinetic movements. It occurs particularly with symptomatic (secondary), as opposed to idiopathic (primary), dystonias, for example, postencephalitic and neuroleptic-induced dystonia, the latter now being the most common cause. This is usually an acute effect but may on occasion be seen as a consequence of chronic therapy (tardive oculogyric crisis). It has also been described with Wilson’s dis ease, neuroleptic malignant syndrome, and organophosphate poisoning. Lesions within the lentiform nuclei have been recorded in cases with oculogyric crisis. Treatment of acute neuroleptic-induced dystonia is either parenteral benzo diazepine or an anticholinergic agent such as procyclidine, benztropine, or trihexyphenidyl. Oculogyric crisis and abnormal magnetic resonance imaging signals in bilateral lentiform nuclei. Fascicular (within substance of midbrain): all muscles or specific mus cles involved, + other clinical signs expected, such as contralateral ataxia (Claude’s syndrome), hemiparesis (Weber’s syndrome). Orbit: paresis of isolated muscle almost always from orbital lesion or muscle disease. Oculomotor nerve palsies may be distinguished as ‘pupil involving’ or ‘pupil sparing’, the former implying a ‘surgical’, the latter a ‘medical’ cause, but this distinction only holds for complete palsies. Transtentorial (uncal) 250 Onion Peel, Onion Skin O herniation due to raised intracranial pressure may, particularly in its early stages, cause an oculomotor nerve palsy due to stretching of the nerve, a ‘false-localizing sign’. In young patients this is most often due to demyelination, in the elderly to brainstem ischaemia; brainstem arteriovenous malformation or tumour may also be responsible. A vertical one-and-a-half syndrome has also been described, characterized by vertical upgaze palsy and monocular paresis of downgaze, either ipsilateral or contralateral to the lesion. Electro-oculographic analyses of five patients with deductions about the physiological mechanisms of lateral gaze. A unilateral disorder of the pontine tegmentum: a study of 20 cases and a review of the literature. It reflects the somatotopic sensory representation in the spinal nucleus of the trigeminal nerve: midline face (nose, mouth) represented rostrally, lateral facial sensation represented caudally. External ophthalmoplegia: weakness of the extraocular muscles of central, neuromuscular, or myopathic origin: Supranuclear: The term ‘ophthalmoplegia plus’ has been used to denote the combination of progressive external ophthalmoplegia with additional symptoms and signs, indicative of brainstem, pyramidal, endocrine, cardiac, muscular, hypothalamic, or auditory system involvement, as in mitochondrial disease. Cross References Coma; Decerebrate rigidity; Emposthotonos Oppenheim’s Sign Oppenheim’s sign is a variant method for eliciting the plantar response, by appli cation of heavy pressure to the anterior surface of the tibia, for example, with the thumb, and moving it down from the patella to the ankle. Extension of the hal lux (upgoing plantar response, Babinski’s sign) is pathological. Like Chaddock’s sign, Oppenheim’s sign always postdates the development of Babinski’s sign as a reliable indicator of corticospinal pathway (upper motor neurone) pathology. Although some normal individuals can voluntarily induce opsoclonus, gen erally it reflects mesencephalic or cerebellar disease affecting the omnipause cells which exert tonic inhibition of the burst neurones which generate saccades. Of the paraneo plastic disorders, opsoclonus associated with lung and breast tumours persists and the patients decline from their underlying illness; neuroblastoma associated opsoclonus may be steroid responsive. Clinical outcome in adult onset idiopathic or paraneoplastic opsoclonus–myoclonus. Cross References Ocular flutter; Saccadic intrusion, Saccadic pursuit; Square wave jerks Optic Aphasia Optic aphasia is a visual modality-specific naming disorder. It has sometimes been grouped with associative visual agnosia, but these patients are not agnosic since they can demonstrate recognition of visually presented stimuli by means other than naming. Moreover, these patients are not handicapped by their deficit in everyday life, whereas agnosic patients are often functionally blind. Objects that are semantically related can be appropriately sorted, indicat ing intact semantics. This is not simply anomia, since the deficit is specific to visual stimuli; objects presented in tactile modality, or by sound, or by spoken definition, can be named. Naming errors are often semantic, and perseverations (‘conduit d’approche’) are common. Perception is intact, evidenced by the ability to draw accurately objects which cannot be named. Optic aphasia is associated with unilateral lesions of the left occipital cortex and subjacent white matter. Visual agnosia: disorders of object recognition and what they tell us about normal vision. A visual-speech disconnexion syndrome: report of a case with optic aphasia, agnosic alexia and colour agnosia. Cross References Anomia; Conduit d’approche; Visual agnosia 254 Optic Atrophy O Optic Ataxia Optic ataxia is impaired voluntary reaching for a visually presented target, with misdirection and dysmetria. Tactile search with the palm and fingers may be undertaken in searching for an object, using somatosen sory cues to compensate for impaired access to visual information. Hence this may be characterized as a modality-specific apraxia, wherein visual informa tion cannot be used to guide goal-directed movements. Optic ataxia occurs with lesions of the intraparietal sulcus and regions medial and superior to it; the primary visual cortex is intact. It is one fea ture, along with psychic paralysis of gaze (‘sticky fixation’) and simultanagnosia (visual disorientation), of Balint’s syndrome in which there is some evidence for parieto-occiptial (and possibly frontal) lobe dysfunction (disconnection). Cross References Apraxia; Ataxia; Balint’s syndrome; Dysmetria; Simultanagnosia; Visual disori entation; Visual form agnosia Optic Atrophy Optic atrophy is pallor of the optic nerve head as visualized by ophthalmoscopy. The temporal disc may appear pale in a normal fundus, so that optic atrophy can only be confidently diagnosed when there is also nasal pallor, although temporal pallor may follow damage to the macular fibre bundle with central visual defects. Optic atrophy may be the consequence of any optic neuropathy which causes optic nerve damage leading to gliotic change of the optic nerve head. Although most often seen with optic nerve pathology, it may be a consequence of pathology in the retina, optic chiasm, or optic tract. In clinical practice a striped drum serves to test both visual pursuit and saccades. Rotation of the stripe to the left produces leftward pursuit, followed by a compensatory saccade to the right, followed by pursuit to the left of the next stripe, with another compensatory saccade, and so on. Clinical and imaging studies show a strong correlation between oro-facial dyspraxia and lesions in the frontal operculum; it may also occur with subcortical lesions involving periventricular and/or peristriatal white matter as well as the basal ganglia. Progressive loss of speech output and orofacial dyspraxia associated with frontal lobe hypometabolism. Normally there is a drop in blood pressure of lesser magnitude on standing but this is usually quickly compensated for by the barore ceptor reflex. Measuring blood pressure automatically by passive head-up tilt testing (tilt table) is also helpful in diagnosing orthostatic hypotension if the active standing test is negative, and the history is suggestive, or in patients with motor impairment. Symptoms which may be associated with orthostatic hypotension include exercise-induced or postprandial light-headedness, transient visual loss (usually bilateral), blackouts (syncope), and pain in a ‘coathanger’ distribution across the shoulders. Cross Reference Hallucination Peek Sign One of the eye signs of myasthenia gravis: on attempted forced eye closure, orbic ularis oculi may fatigue such that the patient ‘peeks’ through the partially open palpebral fissure. Peliopsia, Pelopsia Peliopsia or pelopsia is a form of metamorphopsia characterized by the misper ception of objects as closer to the observer than they really are (cf. Cross References Metamorphopsia; Porropsia Pelvic Thrusting Pelvic thrusting may be a feature of epileptic seizures of frontal lobe origin; occa sionally it may occur in temporal lobe seizures. Pelvic thrusting also occurs in pseudoseizures, particularly those of the ‘thrashing’ variety. Choreiform disorders may involve the pelvic region causing thrusting or rocking movements. Cross References Automatism; Chorea, Choreoathetosis; Seizure Pendular Nystagmus Pendular or undulatory nystagmus is characterized by eye movements which are more or less equal in amplitude and velocity (sinusoidal oscillations) about a central (null) point. In acquired causes such as multiple sclerosis, this may pro duce oscillopsia and blurred vision. Acquired pendular nystagmus in multiple sclerosis: an examiner–blind cross-over treatment study of memantine and gabapentin. Cross References Nystagmus; Oscillopsia Percussion Myotonia Percussion myotonia is the myotonic response of a muscle to a mechanical stim ulus. For example, a blow to the thenar eminence may produce involuntary and sustained flexion of the thumb. This -273 P Periodic Alternating Nystagmus response, which may be seen in myotonic dystrophy, reflects the impaired muscle relaxation which characterizes myotonia. Cross Reference Myotonia Periodic Alternating Nystagmus Periodic alternating nystagmus is a horizontal jerk nystagmus, which damps or stops for a few seconds and then reverses direction. Periodic alternating nystagmus may be congenital or acquired, if the latter then its localizing value is similar to that of downbeat nystagmus (with which it may coexist), especially for lesions at the cervico-medullary junction. Treatment of the associated lesion may be undertaken, otherwise periodic alternating nystagmus usually responds to baclofen, hence the importance of correctly identifying this particular form of nystagmus. Cross Reference Nystagmus Periodic Respiration Periodic respiration is a cyclical waxing and waning of the depth and rate of breathing (Cheyne–Stokes breathing or respiration), over about 2 min, the crescendo–decrescendo sequence being separated by central apnoeas.
This technique should therefore only be used in the Surgical Principle facial region when absolutely necessary depression definition synonyms order amitriptyline without prescription. As an alternative anxiety quiz online cheap 25mg amitriptyline otc, a modi Àed half-buried (Allgöwer) mattress suture can be used (Fig mood disorder treatment 25 mg amitriptyline amex. The advantage of the mattress suture is its safer re-approxima tion of wound edges with di erent depths mood disorder jokes purchase amitriptyline 50 mg line. This suture everts the wound edges and helps avoid “furrowlike” scar formation legitimate depression test generic 50 mg amitriptyline with mastercard. Basic Principles 15 Continuous (Running) Suture Rules depression youtube order amitriptyline in india, Tips, and Tricks 4 Surgical Principle the end of the suture should be held under slight tension by an assistant. On completion, the wound edges should be checked the area of usage of this suture corresponds to that of the inter and, if necessary, everted. Unlike the intracutaneous suture, this suture technique is also Good results can be expected above all in areas of thin and suitable for curvilinear wounds, in which case the stitches should readily mobile skin with few sebaceous glands. In the subcutaneous tissue, entry and exit passage must be the primary management of soft-tissue injuries of the face is made at exactly the same distance from the skin surface. Wounds that are not adequately treat a knot is tied, as with an interrupted suture. Crossing back to the original side, the entry site is at the same intra cutaneous level with a near exit site. Local wound management is the initial scars that lie above skin level but do not extend beyond the treatment for nonurgent bony injuries of the skull; the treat boundaries of the original wound. The tendency to form keloids is often Primary Management of Facial Injuries inherited. Areas of predilection are, among others, the poste Ensure adequate tetanus immunization. Since inconspicuous 5 Check wounds for foreign bodies, consider cleansing and scars, hypertrophic scars, and keloids can coexist in the same irrigation with physiological saline or hydrogen peroxide; patient, the existence of a “normal scar”. Sparingly straighten any jagged wound edges, conservative Standard Operative Techniques for Scar Revision skin excision (no formal wound excision). Re-approximate superÀcially avulsed epithelium with Àbrin Small retracted scars. The operation is per taneous junctions of skin and mucosa (free alar margin, lip, formed under local anesthesia and may be repeated at 4 to eyelid margin). Hypertrophic scars are excised, together with a margin of With dog-bite injuries there are usually full-thickness defects, healthy tissue, if they do not regress spontaneously within commonly in the region of the tip of the nose. Wound tension, which is the cause of the increased pro ing wound, then it may carefully cleaned and primarily closed duction of collagen, must then be reduced. Attempts should be made to reconstruct such defects jacent tissue must be widely undermined to make it possible early (within 24 hours after sterile dressing) with appropriate to approximate the wound edges under minimal tension. Scar contracture after second main tension must be taken up by absorbable subcutaneous su ary healing requires generous excision and undermining of tures (see Figs. Management of Keloids Scar Revision the management of keloids is problematic, given that they are neoplastic growths initiated by injury to the dermis. Any skin Scar revision may be indicated for functional reasons if severe incision made for scar revision will therefore induce the forma contractures and distortions are present. Further measures are taken as prophylaxis against recurrence (see be Questions to Ask in the Preoperative Assessment low). Intralesional injection of the revised wound with a pen, ensuring that the lines of either side interdigi with a steroid crystal suspension, followed by weekly repeat injec tate. In addition, pressure dress the previously marked skin is scored with a pointed scalpel ings should be applied for as long as possible (depending on the blade (No. Should the result the scar is then excised with the scalpel, producing vertical ing defect after excision of the keloid be too large for primary incisional edges down to the subdermis. The triangular skin Áaps are repaired with Àne sutures 5 lar may be treated with a skin graft harvested from the groin. The indication for the revision of keloid scars should be made with extreme caution and the patient should not be encouraged to be too optimistic about the prospects of success. Rules, Tips, and Tricks the triangular skin Áaps should not be cut too small and should W-plasty be raised from unscarred skin. The area of undermining depends upon the resulting defect: it should at least equal the width of the Surgical Principle defect on either side. This undermining of the skin is the simplest method for dealing with skin tension. A few skin sutures for ap Converting a linear scar into a zigzag shape distributes the proximation are helpful before placing the deÀnitive skin suture, tensile forces in the region of the scar so that the scar line is so as not to misjudge each corresponding Áap and be left with a optically “broken up. At the same time retracted scars are corrected by resection and Alternatives undermining. Unlike the regular M or W-shaped scar formation after W plasties, the geometric broken-line technique results rather Indications in a scar that is broken up and rendered less conspicuous. Note the incision along the wound edges where largely congruent surfaces are created. Formation of identical geometric forms on either side of the scar (not mirror images). The mobility of the lateral skin should be taken into consider Surgical Principle ation when planning the operation (remember aesthetic units). Tension between the ends of the scar is relieved (a scar which is “too short” is lengthened). Surgical Principle Indications the technique achieves lengthening of the scar (without trans For any scar revision, it is above all the lengthening and trans position) by linear advancement. The nomenclature comes from the initial V-shaped at the expense of the adjacent lateral tissue (see arrow in Fig. The lateral skin is undermined to create lateral limbs at the end of the wounds and two trian and the opposite end of the wound is placed under tension with gles are elevated by undermining. Rules, Tips, and Tricks Maximal gain in length with reorientation of the scar by 90° is Rules, Tips, and Tricks only achieved if the length of the lateral limbs corresponds to the No new distortions should appear in the lateral regions of the length of the scar and they are at an angle of 60° to the scar (for wound; if necessary, the undermining should be extended. Because of their Adherent Scars thickness, preference should be given to skin Áaps to cover deep-seated defects. The simple excision and primary closure of extensive scars or other skin lesions. The re sulting defect must then be resurfaced either with a Áap or a Management of Soft-Tissue Defects skin graft (see below). This involves removing General Remarks only a part of the area, with dimensions such that a primary wound closure is just about possible. This allows the skin lesion Soft-tissue defects can be managed with either pedicle Áaps or to be excised gradually in several sessions. Pedicle Áaps are attached to the adjacent tissue by a paid here to the site of the resulting scar, any potential distor bridge of tissue, in which the feeding vessels run. Usu directly after excision because of the lack of mobility of the ally other Áap procedures are available to resurface defects of adjacent skin. Here too, plastic reconstructive procedures us the head and neck region, which will achieve the desired result 20 5 Reconstructive Plastic Surgery of the Face 1 4 5 a Fig. Because indications for their use in the facial region are limited, vascular pedicle Áaps are not dealt with any further here. Preliminary Remarks Another possibility for facilitating the creation of skin Áaps is to produce excess tissue in the vicinity of the defects by skin Pedicle Áaps are named according to the type of Áap movement expansion; the excess skin created in this way is then recruited (linear advancement, rotation, transposition) and their pedicle. The procedure requires a certain amount of preparation In the following, a distinction will also be made within these time and is not as easily employed in the region of the face as in two groups according to the type of Áap movement. Basic Principles 21 gen deÀciency; rather, it is due to a dilation of the shunt vessels Rules, Tips, and Tricks caused by the autonomic nervous system. Flap delay is always 4 Aspects regarding the planning of Áaps: recommended when the size of the Áap exceeds a length-to Size of the defect vs. It is important to pay attention to the direction of the greatest the length of these Áaps depends on the position of the feed gain in tissue length (line connecting the base of the Áap and ing vessels, and the width depends on the dimensions of the 4 the furthest edge of the defect). In comparison with random pattern Áaps, these Áaps have the disadvantage of only being available in certain areas. Typical examples are the paramedian forehead 5 Áap (supratrochlear artery), the cheek Áap (facial artery), the Size, Blood Supply, and Viability of Pedicle Flaps temporal Áap (superÀcial temporal artery) and, as an important example of a pedicle Áap from the chest region for covering de As described above (p. All over the body, the subdermal plexus is (branches of the internal mammary artery). These are dis axial pattern Áaps may be supplemented at their tip by a ran tributed randomly and allow the elevation of skin Áaps of lim dom pattern Áap, resulting in Áaps that receive their blood sup ited size (random pattern Áaps). When the dimensions of Because skin of the face has a better blood supply than other the Áap are borderline, as local conditions often dictate, addi regions of the body, facial Áaps may, however, be twice as long tional risk factors, such as smoking, may put its viability at risk. The actual blood Áow to Pinpoint bleeding at the cut edges of a Áap can be regarded as a the periphery of the Áap depends on whether the perfusion sure sign of an adequate blood supply. This resistance may when, after a brief application of pressure to the Áap, the skin be high in a scarred or previously irradiated area, for example, Àrst appears livid and then regains its normal color within sec so that widening the Áap pedicle may indeed increase the num onds. If Áap necrosis is anticipated, the the feeding vessels belong to the same Áow system. After 2–3 weeks the deÀnitive Áap elevation Flaps with an Intact Epithelial Surface and transfer may be completed. However, scar formation will have already begun and this will limit the degree of modeling of Flaps of this type are summarized in Fig. If the base of the Áap becomes too 1 the simplest type of linear skin advancement is the extensive narrow, however, there is a risk of Áap necrosis. If there is a more signiÀcant degree of Special Forms tension, then the contact area of the sutures may be enlarged by plastic disks or gauze pledgets (dental rolls) (Fig. Ad Rhomboid Áaps are based on the geometrical concepts of Du vancement Áaps which have been elevated on three sides (Fig. One special type is the V–Y plasty, A rhombus-shaped incision should be planned for the ex which has already been discussed (Fig. The defect is Àrst resurfaced with a rotation Áap from an adjacent region with only poorly mobile skin. The resulting donor defect is covered with a transposition Áap from a region with readily mobile skin. The elasticity of the skin is used to advantage: the Àrst Áap is slightly smaller than the defect, with the second Áap be ing smaller again than the Àrst. Multiply lobed Áaps are theoretically possible, but the option can usually be restricted to only two Áaps. A typical usage is the resurfacing of a defect on the dorsum of the nose, with the pri a b mary Áap recruited from the immediate vicinity and the second Áap coming from the glabellar region. Transposition Áaps have a partial bridge of tissue between re b Appearance after wound closure. Flap Limberg: the short diagonal b–d is extended; distance e–d = a–b; e–f transposition and wound closure are identical for both techniques. It should be kept in mind, gion of the nose (nasolabial Áap, paramedian forehead Áap, see however, that the more the Áap is rotated the shorter it be Fig. Because dog-ears may develop at the base of the Áap, a the Z-plasty, a further example of a transposition Áap, has second operation is often required for deÀnitive management of already been mentioned (see Fig. The base of the Áap may be contoured about 3 weeks Apart from these local transposition Áaps, there are also after transposition by excision and thinning out. The best known are Conley’s chest Áap and 24 5 Reconstructive Plastic Surgery of the Face Fig. They are mainly used as distant in the thorax, they can be used as long axial Áaps to cover de Áaps, i. The development of new several intermediate steps to the recipient site, when no suit techniques—especially the rediscovery of the pectoralis major able epithelium is available in the vicinity. They have not completely sunk into oblivion, however, because in special cases their reliability sometimes o ers a way out of an other Hinged Turnover Flap (Fig. Hinged turnover Áaps are intended for the coverage of through and-through defects, where transposition of the Áap no longer Flaps without a Continuous Epithelial Surface takes place at skin surface level, but rather the Áap is turned over 180° around an axis that lies level with the skin. The bilateral blood supply means that the arteries and veins when dissecting the pedicle, to prevent relatively long Áaps may be raised, which can consequently injury to the vessels. Advantages include the possibility of a one-stage approach and the avoidance of larger scars. The thoracoacromial artery runs beneath the clavicle sected and palpated in the loose connective tissue. Excessive restriction of blood Áow to the Áap by rotation or Indications twisting of its pedicle is a risk. The Áap pedicle extends from the nipple to the clavicle and al lows a large arc of action, reaching as far as the cheek region (Fig. Thus, for example, skin defects of the parotid re Special Form: Pectoralis Major Myocutaneous Island Flap gion after radical parotidectomy can be treated, or defects of the Áoor of the mouth after tumor excision. The vascular supply Surgical Principle of this Áap is very good, allowing it also to be used for defects this Áap consists of a skin island, the nutrient artery of which in irradiated areas. Because of its size, the Áap is well suited for (the thoracoacromial artery) runs in or under a muscle pedicle resurfacing larger defects, including full-thickness perforation (pectoralis major muscle). The Áap pedicle therefore incorpo defects of skin and mucosa, as well as for soft-tissue volume rates this muscle, and the size of the skin island can almost replacement (Áoor of the mouth, tongue). The donor site can be muscular Áap pedicle is a disadvantage and needs to be rotated closed primarily. In everyday language, the term “transplant” is used without a clear distinc tion. Because grafts do not have their own blood supply, they depend After incision of the pectoralis major muscle by blunt dis upon the conditions prevailing at the recipient site for their nu section, the vascular pedicle is identiÀed beneath the fascia trition. After ap An incision is made around the muscle at the distal circum proximately 10 days the graft is Àrmly adherent to the recipient ference of the skin island (the thoracoacromial artery runs bed. Fresh wounds are usually unsuitable for primary grafting, vascular damage by shear movements) (Fig. Secondary coverage, after the muscle pedicle is dissected with division from the main the formation of a Áat layer of granulation tissue, is more fa muscle (preferably using an electric knife) approximately vorable.
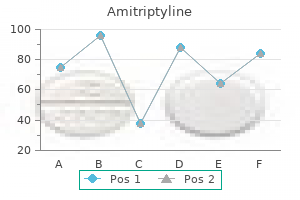
In some complex programs these requirements partially depend on the duration of missions depression definition oxford dictionary discount amitriptyline online amex, with the range of screening and monitoring modalities increasing with flight duration depression zodiac signs buy 25 mg amitriptyline free shipping. Within a particular program bipolar depression 35 purchase 25mg amitriptyline visa, medical monitoring modalities can still largely vary depending on the features of the particular mission depression cherry review purchase 50 mg amitriptyline visa. For example depression symptoms signs trusted amitriptyline 25mg, mission-specific pre and postflight monitoring modalities can depend on mission 3 V 4 Ch 3 Medical Monitoring Before and After Flight Billica et al mood disorder medication cheap amitriptyline 25 mg online. The individual pre and postflight monitoring plan is composed by the crew surgeon on the basis of program specific requirements, mission-specific factors, individual mission assignments as well as data on the individual’s responses to the previous missions, particularities, and the speed of recovery and rehabilitation processes. Real-time corrections to the individual pre and postflight monitoring program are also possible at any time to relieve any concerns of the crew surgeon. Individual Baseline Databases Health monitoring data collection is planned at fixed intervals in conjunction with the physical health evaluations at astronaut selection and before the first mission; they collectively establish a baseline normative database against which in-flight management and postflight recovery will be implemented. Prior experience has demonstrated significant diversity of individual physiological responses to space flight factors; in particular, it is believed important to establish a baseline profile for each crewmember in terms of metabolic and endocrine functions, and 19 electrolyte and acid-base balance ; prior experience has demonstrated significant diversity of individual 3,19,20 physiological responses to space flight factors. During subsequent missions, depending on available information and the clinical judgment of the crew surgeons, only select protocols may be implemented if adequate baseline data already exist. The established baseline may be re-established periodically, as clinically indicated. In the postflight phase, guided by clinical manifestations and physical evaluation, only those protocols can be implemented that are required for diagnostic purposes or to guide the rehabilitation process and the return to flight duties. Preflight Medical Evaluation and Monitoring Activities Medical fitness for flight is determined by the crew surgeon, who conducts preflight medical evaluations of all crewmembers. In Russia, data obtained from cosmonauts’ physical examinations are reviewed by the Main Medical Board of the Ministry of Public Health and the Ministry of Defense of the Russian Federation 45 days before space flight. Depending on the nature and duration of the flight, there are minimum sets of tests/examinations required at certain intervals referenced to the launch or landing date. In Russia, this is conducted in accordance with regulations put into effect by an Order from the Minister of Public Health and the Minister of Defense (see Chapter 1). The International Space Station Program has adopted most of the principles of preflight medical evaluation and monitoring that have been verified during various programs conducted by space, military, and civilian agencies in several countries, primarily the United States and Russia. Skylab and Space Shuttle programs and the Russian long-duration space flight experience aboard the Salyut and Mir stations are the main sources of current knowledge in this area. Significant contribution to the knowledge base of space medicine monitoring has been made by ground-based experiments and simulations. As described in Chapter 1, astronaut candidate finalists undergo thorough 5-day physical and laboratory exams, including a treadmill stress test; pulmonary function tests; sigmoidoscopic and imaging examinations; and exams conducted by specialists in ophthalmology, neurology, psychiatry, dentistry and otolaryngology. After selection, astronauts undergo yearly medical examinations to recertify their fitness for flight. This training includes familiarization with the medical and physiological problems encountered in microgravity, including space motion sickness, cardiovascular deconditioning, reduced-pressure effects and decompression sickness, radiation, habitability and countermeasures, and use of in-flight medical equipment. Two crewmembers are designated crew medical officers and receive additional training in diagnosing and treating common medical problems, administering intramuscular and intravenous medications, and using onboard clean-up kits for decontamination and protection from potentially hazardous contaminants. Crew medical officers are equipped with a “medical checklist,” a quick reference to common ambulatory and emergency medical problems and a complete description of all onboard medications and their side effects. All crewmembers undergo extensive preflight medical examinations in addition to those associated with biomedical research and longitudinal data collection. Preflight exams, typically scheduled 10 days and again 2 days before launch, are conducted to detect any medical problems that might require attention and to provide baselines for postflight comparison. Results from these examinations are compared to those from two postflight sessions held the day of landing and three days thereafter. In addition to the certification process, astronauts also undergo real-time medical monitoring during potentially hazardous activities, such as underwater and hypobaric-chamber training sessions and some forms of biomedical testing. Medical staff oversee all potentially hazardous activities as a means of ensuring safety and quality assurance. Russian Program Cosmonaut selection and training are considered to be an integrated, continuous process. The goal of the outpatient phase is to identify overt pathology and functional disorders that would represent absolute contraindications for space flight (Table 1). Examinations in the hospital are designed to identify latent (occult) pathology, incipient preclinical forms of disease, and slight deviations in the functional status of organs and systems, as well as to evaluate physiological functional reserves. Candidate cosmonauts undergo comprehensive assessments by internists, surgeons, otolaryngologists, dentists, neuropathologists, and psychologists. Special provocative tests also are used to evaluate the “reserve potential” of the physiological system being tested. The results of these tests and evaluations, and those from tests conducted after cosmonauts are assigned to a crew (see below), are assessed by the Medical Certification Board, which declares individuals either qualified for special training, qualified with reservations, or not qualified (see Chapter 1). Qualification with reservations usually reflects the discovery, during the evaluation process, of a medical condition that requires treatment; such individuals are deemed temporarily unfit for special training for up to 6 months. Individuals who pass the inpatient testing stage subsequently undergo special training (see Chapter 2), the goals of which are to improve tolerance and induce adaptive physiological reactions to specific space flight factors, and to impart the skills needed to control spacecraft systems and equipment. If a cosmonaut has a health problem that requires clarification or reassessment of the Board’s recommendation, then a special examination and Board session are held. Other medical assessments conducted between regular Board meetings (during the training process) are observations during tests, physical training and daily life; interim medical examinations; and quarterly in-depth medical examinations. Interim examinations (Table 2) are held before and after any training procedure that makes unusual demands on cosmonaut health. Interim exams including analysis of blood and urine, and evaluations by internists, neuropathologists, and 5 V 4 Ch 3 Medical Monitoring Before and After Flight Billica et al. If the results of preliminary interim examination are positive, the cosmonaut is allowed to participate in further tests and training. Results of the last interim examinations are used to assess the effect of training on the cosmonaut’s health and tolerance of the factors to which he or she has been exposed. Measures are taken as needed to improve physiological tolerance of particular factors. In-depth examinations (also conducted as part of the outpatient selection process) take place quarterly (Table 3). These examinations include general clinical analyses of blood, urine, and feces; cosmonauts older than 40 years also undergo tests of blood sugar and cholesterol every 6 months. Cosmonauts also are examined by specialists in internal medicine, neuropathology, surgery, otolaryngology, ophthalmology, and dentistry. Results from medical and psychological observations and from interim medical examinations during training also are considered during the in-depth examination. Tests for recertification closely resemble those of the inpatient selection phase (Tables 4 and 5). Cosmonauts undergo additional clinical and physiological tests once before they are assigned to a prime or a back-up crew, again 30 to 60 days before launch, and again 5 to 7 days before launch. When an individual is assigned to a crew, results from the last regular inpatient certification can be used if the Board finds no reason to repeat any of the component tests. The tests constituting preflight examinations are similar to those of the annual recertification but include 24-hour Holter monitoring and assessments of tolerance of low atmospheric pressure and +4 to +8 Gx accelerations. The different acceleration profiles used for annual versus preflight certifications reflect the different goals of the two processes. The annual test (tolerance of +3 Gz and 5 Gz for 30 seconds each) seeks to evaluate general tolerance and allows cosmonauts to begin flight training. Preflight certification tests (tolerance of +4 to +8 Gz) seek to predict individual tolerance of acceleration profiles expected during actual space flights. Good tolerance of transverse (+Gx) acceleration (magnitude up to 8 G, duration up to 40 seconds) has been shown to predict good tolerance of acceleration during the active phases of flight on Soyuz-type spacecraft, including emergency ejection and descent from orbit. Conditions such as contusions (with limited tissue edema), minor cuts or bruises, limited 1 or nd 2 -degree burns or frostbite, single boils that are not associated with fever or do not affect the individual’s general state, or acute infectious laryngitis and pharyngitis (without severe symptoms of toxicity) are generally treated on an outpatient basis. After either inpatient or outpatient treatment, a short period of rest (not longer than 15 days) may be prescribed, during which the cosmonaut cannot participate in training. When the recovery and rest periods are over, the cosmonaut resumes classroom work first and then special training. The final preflight medical examination takes place 5 to 7 days before launch and again on the day of launch. Launch-day evaluations are conducted by internists, neuropathologists, and otolaryngologists. Scientific studies and experiments are conducted independent of the preflight medical evaluations. These studies are conducted in accordance with special programs developed before each flight, and theoretically can include experiments in any area of physiology, medicine, pharmacology, hygiene, or psychology. The results from such studies, like those from baseline medical monitoring, can be significant in the flight certification process, although they are not a mandatory part of the decision making. At this time, a crew surgeon, deputy crew surgeon, and biomedical mission manager are assigned to the mission. Further medical data reviews and monitoring activities become the responsibility of the crew surgeon. This individual schedules and arranges for every evaluation, assessment, data sampling, and other activities. The crew surgeon ensures that all existing monitoring and preparatory requirements are satisfied and that each individual crewmember’s medical records precisely reflect all acquired information. Six months before the scheduled launch date, the crew aeromedical summaries and drug sensitivity testing records are updated. Nutritional assessment and counseling, and radiation history reviews are required at this time, and individual exercise programs are initiated. One month before launch, the crew surgeon and deputy crew surgeon meet with the crew for medical examinations and preflight medical testing to include a full flight physical examination. For short missions (less than 30 days), this session replaces the medical evaluation held 10 days before launch. Further medical examinations fall into the category of “near-flight” exams (L–10 days or closer). These evaluations are conducted at the launch site or at the training site before crew transfer to the prelaunch crew quarters. Near flight examinations are conducted to detect any medical problems that might require attention and to provide “fresh” baselines for postflight comparison. A comprehensive preflight examination is performed 10 days (for short flights) or 7 days (for intermediate or long flights) before launch. Additional studies commensurate with the annual evaluation’s requirements may be added so that this exam, if performed within 30 days of the crewmember’s birthday, will substitute for the annual exam. For short flights, this preflight medical evaluation consists of a full physical, otolaryngology and ophthalmology evaluation, cardiovascular/cardiopulmonary studies, a battery of laboratory tests, and microbiological assessments (Table 6). For long flights, nutritional assessment and repeated microbiological sampling are required. Findings are released on the crew’s health status, and this is equivalent to confirming that the crew is flight-ready. On launch day, a brief medical evaluation (several minutes long) takes place on the launch site, which terminates the preflight medical evaluation and monitoring sequence. Results from these preflight examinations are later compared to those from the postflight sessions on the day of landing and three days thereafter. After “main engine cutoff,” the crew surgeon and deputy crew surgeon return to the Johnson Space Center to begin the in-flight portion of crew medical monitoring. For a launch from Russia, the procedures for examining the crews are in keeping with the “final preflight examinations” program described above in the “Russian Program” section. Russian Program As noted earlier, the difference between medical assessment/certification and preflight countermeasures is somewhat blurred in the Russian space program, since training is considered an extension of the selection and assessment process. The primary goal of the general training is to improve cosmonauts’ physiological tolerance of space flight factors as they acquire new occupational and professional skills. Traits revealed during training, such as speed and stability of an individual’s adaptive responses, are important in evaluating a candidate’s performance. For this reason, the provocative tests used during this phase simulate space flight factors as closely as possible. Special attention is given to cosmonaut-researchers (payload specialists) during this training so that their performance and abilities can be expanded as much as possible. Some means by which general conditioning is improved have 7 V 4 Ch 3 Medical Monitoring Before and After Flight Billica et al. As the durations of space flight continue to increase, it becomes apparent that maintaining the adaptive capacities of crewmembers during those flights will necessitate the development of additional prophylactic countermeasures that can be used both during preflight training as well as during actual missions. Program Many preflight activities have been implemented to protect crew health before launch and to prevent medical problems that could delay or impair missions. The Health Stabilization Program was designed to minimize crew exposure to infectious disease before missions. The brevity of early Mercury and Gemini flights was such that the possibility of infectious diseases manifesting themselves during flight was not considered a concern. As the duration of the Gemini flights increased, the corresponding increase in risk of disease prompted reducing the number of people to whom the crews were exposed before launch. Although no serious episodes took place during flight, Gemini crews did experience minor illnesses such as colds and influenza during the period before launch. During the Apollo program, concern increased over the possibility and consequences of infectious diseases, particularly with regard to the difficulty of completing a lunar landing should a crewmember become seriously ill during the mission. During preparations for Apollo-8, every crewmember suffered viral gastroenteritis during the preflight period. However, the recurrence 28 of the infection in one crewmember during flight greatly increased awareness of the need for more stringent preflight measures to protect astronaut health during missions. The Apollo-14 mission was the first to be conducted under a formal Health Stabilization Program for flight crews. The goal of this program was to eliminate in-flight health problems by minimizing or eliminating adverse alterations in the health of flight crews during the period immediately before launch.
Generic amitriptyline 50mg without prescription. The Symptoms of General Anxiety and Panic Disorder.
References
- Borno ST, Fischer A, Kerick M, et al. Genome-wide DNA methylation events in TMPRSS2-ERG fusion-negative prostate cancers implicate an EZH2-dependent mechanism with miR-26a hypermethylation. Cancer Discov 2012;2(11):1024-1035.
- Levey S, Jennings ER: The use of control charts in the clinical laboratory, Am J Clin Pathol 20:1059, 1950.
- Thompson G, Stevenson GW, Somers S. Distribution of gastric ulcers by double-contrast barium meal with endoscopic correlation. J Can Assoc Radiol 1983; 34:296-297.
- Zelefsky MJ, Cowen D, Fuks Z, et al: Long term tolerance of high dose threedimensional conformal radiotherapy in patients with localized prostate cancer, Cancer 85(11):2460n2468, 1999.
- Yamashita T, Ogawa A: Ultrasound in penile cancer, Urol Radiol 11:174n187, 1989.
- Piovella F, D'Armini AM, Barone M, VF. T. Chronic thromboembolic pulmonary hypertension. Semin Thromb Hemost 2006;32:848-855.

