
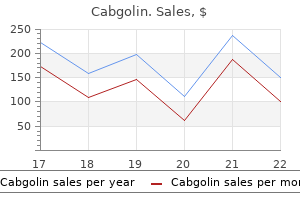
Walid Al-Wali MBChB FRCPath
- Professor of microbiology, Consultant
- medical microbiologist, Lead infection
- control doctor, Director for infection
- prevention and control, Medical director
- Department of Medical Microbiology,
- Rotherham NHS Foundation Trust,
- Rotherham, UK
If ac botulinum toxin A or muscle lengthening procedures may tive supination is absent medications after stroke cheap cabgolin 0.5mg amex, but free movement is possible resolve this problem treatment centers in mn order cabgolin once a day. Osteotomies and arthrodeses have passively symptoms 8dpo order cabgolin no prescription, transfer of the pronating muscles is indicated treatment restless leg syndrome discount cabgolin 0.5mg without prescription. If movement restriction without pronatory activity is Flexion contractures at the elbow are relatively com present symptoms 6 days before period purchase cabgolin on line amex, the pronator quadratus is lengthened and can be mon symptoms jet lag order cabgolin canada. However, since these are usually slight or moderate, transferred at a later date (Table 3. The results and as long as they do not hinder the patient, surgical are better after transfer than after lengthening. Nocturnal splints can be used for alternative to muscle weakening by surgical lengthening is patients with significant progression of the contractures. We have only encountered very troublesome flexion con For fixed flexion deformities of the wrist or a concur tractures in severely tetraspastic patients. Elbow extension rent troublesome instability, an arthrodesis of the wrist orthoses are difficult to use, particularly if spastic counter can produce good results. In such cases, the injection of botulinum this procedure can also be employed for young patients toxin A can slacken the countertension. In addition to the prona to distinguish between a contracture that is merely func tion-flexion position of the wrist, the whole hand is often 489 3 3. Braces can be used to prevent and improve flex the simple Green operation combined with procedures for ion contractures. No negative results have surgery, however, and severe finger deformities persist, been noted to date. In the swan-neck deformity of the operations for correcting the finger function and position fingers (see above) it is usually sufficient to correct the must be considered as a supplement to the transfer of the wrist contracture. In severe cases, a release of the pronator flexor carpi ulnaris muscle (Table 3. Muscle surgery is gener the options for correcting the adduction-pronation ally inadvisable in patients with athetotic atactic-dystonic deformity of the thumb are listed in Table 3. Protocol for the treatment of pronation vative measures tend to be more appropriate than surgical contracture. It is technically Functional deficiency Surgical treatment difficult, however, to provide sufficient stability by internal Active supination bey No operation fixation until the arthrodesis has consolidated. In one pa ond the neutral position tient, for example, we have had to stabilize a wrist arthrod Active supination up to Release of the pronator quadratus esis with two plates instead of just one. Since then the arthrodesis has No active supination, Transfer of the pronator teres consolidated to produce a good end result (Fig. No active supination, Release of the pronator quadratus passive supination re muscle with aponeurotic lengthen Patients undergoing surgery for purely cosmetic reasons stricted or stiff ing of the flexors, poss. However, the more proximal the lesion, the more likely abnormal sprouting will occur. Clinical features and diagnosis Initial signs and symptoms Sensation and motor activity can be tested in older chil dren and adults. The striking finding in neonates is a fail 3 ure to move the arm, which hangs limply with the elbow extended and does not even move when the typical infant reflexes are elicited. If the lower cervical roots are also involved the grip movement of the hand is absent. In the more common upper plexus lesion (Erb-Duchenne) the roots of C 5 and C 6 are affected. Examination of motor function reveals the absence of abduction and external rotation at the shoulder, elbow flexion and, to some ex tent, elbow extension, supination and wrist extension. Wrist arthrodesis in severe athetosis impairment that does occur is located on the outer aspect of the upper arm and the radial side of the forearm. The small surgical procedures on the upper extremities should be hand muscles show no activity and the ulnar fingers, in indicated more liberally, subject to the requirement that, particular, adopt a claw-like posture. But the long finger as with all functional procedures, reliable and adequate flexors and wrist flexors may also be weak or inactive. A Horner syndrome (ptosis, myosis, enophthal mos) may also be present, indicating the involvement of 3. Besides these Plexus palsy two typical clinical pictures, a total arm plexus palsy or other forms of plexus palsies (involvement of C 7 or fas > Definition cicular palsies) may also be present. A plexus palsy refers to a nerve lesion between the point With the aid of an electromyogram, a distinction can at which the spinal roots leave the cord and the point be made between a complete and incomplete paralysis and where they divide to form the peripheral nerves. If deficient movement is present in the upper limb, Etiology and pathogenesis the differential diagnosis must first rule out other injuries Plexus palsies of the upper extremity can occur at birth (fractures of the humerus or clavicle or infections in the as a result of manipulations. Older children and adults can Late sequelae suffer plexus lesions of the upper, or more rarely the lower, Pareses due to birth trauma are typically followed by the extremity in traffic accidents (particularly motorcycle ac development of a muscular dyskinesia at shoulder level, cidents) [15]. No basic distinction is made between plexus where abduction occurs rather between the scapula and lesions in the neonate and the adult [17]. At the same time, not completely severed or torn, the axon will regrow from flexor activity is triggered in the arm, leading to flexion 491 3 3. They also involve the risk of shoulder sublux by altered motor neuron activity, abnormal sprouting or ations, particularly if there are deficits in the muscles that by the abnormal development of the maturing nervous stabilize the shoulder. This procedure is indicated if there are no signs of tracted, usually in a position of internal rotation/adduc a recovery of motor or sensory function by the end of 3 tion. The surgical options include neurolysis, direct opment of bone deformities as a result of the modified suturing or a nerve interposition, and neurotization. The glenoid flattens out and rolysis is indicated if pain is present or, to a lesser extent, becomes broader, while the physiological retrotorsion at in order to improve function. This leads to posterior sub severed, nerve suturing, possibly with the interposition of luxation. The prognosis is better for as a result of hyperactivity of the biceps and brachialis the upper roots than the lower roots, and this also applies muscles and the use of the elbow in a flexion position. Neurotization may be indicated olecranon and coronoid process become enlarged and ad in the event of root avulsions. Lower palsies mainly of elbow function with this method is good (> 50% of affect the hand muscles only. Treatment and prognosis Any subsequent corrective operation must be preceded the prognosis for an upper plexus palsy is better than that by a careful investigation of the functional disorders and for a lower palsy. Overall, over 90% of cases of postpartal deformities and the resulting impairment to the patient. Troublesome eters include the effect of substantial force, complete pal functional deficits can be improved by muscle transfer sies, additional injuries and pain. The latter is indicative procedures, and existing contractures must be eliminated of a root avulsion. The sensory functions recover much beforehand or at the same time with a muscle transfer better than the motor functions. Conservative treatment External rotation and abduction of the arm can be In view of the inherently good prognosis, the primary improved by transfer of the levator scapulae to the supra goal of treatment must be to prevent the onset of second spinatus and relocation of the teres major, with or without ary deformities as these will restrict the function of the the latissimus dorsi, to the infraspinatus muscle. Training of the trapezoid can also be transferred to improve the shoulder existing and newly innervated muscles is also helpful. In addition, there may be posterior or anterior In order to promote the best possible healing, the arm is subluxation or dislocation of the humeral head. From this position, otomy of the proximal humerus in the direction required the muscles are stretched and the existing muscles acti to center the joint [23]. The method according to Vojta is also be used as a replacement for the deltoid [17]. If severe often used for these palsies, but this should probably aim and troublesome instabilities are present, an arthrodesis at strengthening the existing muscles rather than promot of the shoulder may be indicated. The extent to which such stimulation is important for any functional use of the arm. The latis treatments actually produce a positive effect on axonal simus dorsi can also be used to improve elbow flexion. Orthoses and braces can be used, at best, as braces if A precondition for this procedure is a free pronation/su no recovery occurs in the long term and the contracture pination movement. A posterior radial head A curative procedure is suturing of the damaged nerve, dislocation can also occur, and this can be corrected by possibly with an interposed graft. The prognosis is bet radial shortening (in younger children) or a radial head ter, the more distal the lesion, the smaller the damaged resection (in older children). Thumb opposition can be section, the younger the patient and the shorter the pe restored by transferring the flexor digitorum superficialis riod that elapses until treatment. Palliative surgical procedures include muscle transfers and stabilizing measures such as arthrodeses or tenodeses. Etiology and pathogenesis Before any operation the functional deficits and the degree Peripheral nerves are injured in accidents, as the result of of handicap must be clarified and the expectations dis deliberate harm or iatrogenically following their acciden cussed with the patient (Chapter 3. If radial nerve pal tal severing at operation or traction exerted, for example, sy is present, wrist extension can be improved by transfer during the course of corrective axial and lengthening ring the pronator teres muscle to the long and short radial procedures on the extremities. In a median nerve palsy the deficit interferes sation and motor function in the area supplied by that with finger flexion and thumb opposition. The signs and symptoms in typical areas enable pronation of the thumb can be restored by transferring the the damage to be assigned anatomically to the individual extensor indicis muscle, and adduction by relocation of the nerves (Chapter 2. The sensory impairment can be extensor carpi radialis brevis muscle in combination with a present in the form of anesthesia, hypoesthesia, paresthe thumb metacarpophalangeal joint arthrodesis. A distinction lis, although this will result in a loss of power in respect must be made between prognostically favorable incom of fist closure. The pinch grip must be restored with ad plete paralyses and complete failures with anesthesia and ditional measures such as a metacarpophalangeal joint complete paresis. A spontaneous remission can generally arthrodesis of the index finger and transfer of the extensor be expected for incomplete lesions. In any muscle paralysis, however, only over time will it become apparent transfer procedure, however, the surgeon must weigh the whether function will recover or whether the deficit will loss resulting from the removal of the muscle against the persist unchanged. The goal of treatment is to give the patient as much Treatment and prognosis independence as possible. Although the range of motion Conservative treatment in the joints can often not be increased, it can be relocated the orthopaedic treatment is primarily aimed at pre so that the use of the extremity can be improved. At the serving mobility and avoiding contractures so that the same time it may prove necessary to treat both upper muscles can resume their function under the optimal limbs asymmetrically in order to bring one side more in conditions. The main focus of conservative measures is on extension and the other more in flexion. This can help exercise-based treatments in the context of occupational restore the functions needed for eating and personal hy therapy and/or physiotherapy. Contractures and muscle weakness at the shoulder and strengthening exercises, training is provided in the are often present concurrently. Braces can be helpful however, tend to be present only in cases of fixed internal for avoiding contractures. Moreover, functional orthoses rotation, because the arm can no longer be controlled in a can make up for lost muscle functions. In older children or in cases of more pronounced defor Contractures at the elbow can progress in a variety of mity, reconstructive procedures on the skin and corrective ways. Whereas some patients respond well to conserva osteotomies on the metacarpals may also be required. For tive measures, the deformity becomes progressively worse pronounced contractures, the necessary lengthening of the in others, ultimately resulting, for example, in a flexion muscles can be achieved by bone shortening, either by a contracture at the elbow with movement around the right shortening osteotomy of the forearm or by resection of the angle, but with sufficient power remaining in the biceps proximal row of carpal bones. On the other hand, the elbow may stiffen Post-polio syndrome in an extended position, which can significantly interfere On the upper extremity, the deltoid is the muscle most with everyday functioning. In these cases, lengthening or commonly affected in this disorder, although the muscles transfer of the triceps brachii muscle, possibly combined of the rotator cuff may also be paretic and possibly lead with a flexor reconstruction, may be indicated. Troublesome disloca Often a severe flexion contracture at the wrist will tions require an arthrodesis to stabilize the joint. At the already be present at birth, and sometimes fingers and elbow, both flexors and extensors can show weaknesses thumb are also affected. Measures to correct this deformity while, at hand level, thumb opposition in particular is must be initiated as soon as possible, with stretching exer impaired. At a later stage, the wrist instability, and particularly the lack of dorsal flexion, will present a major References problem. Autti-Ramo I, Larsen A, Peltonen J, Taimo A, von Wendt L (2000) Botulinum toxin injection as an adjunct when planning hand improve the functioning of the hands (Fig. A wrist arthrodesis can produce positive effects L (1991) Use of the Green transfer in treatment of patients with and provide stability in the corrected position. Brunner R (1995) Veranderung der Muskelkraft nach Sehnenver level, a distinction must be made between joint contrac langerung und Sehnenverlagerung.
The anaemia is not usually A sex-linked treatment quietus tinnitus buy cabgolin 0.5 mg with visa, hereditary abnormality in which severe medicine 223 purchase cabgolin toronto, but in some instances there is a need for the activity or stability of the enzyme glucose-6 frequent transfusions symptoms non hodgkins lymphoma cheap 0.5mg cabgolin mastercard. Drug-induced haemolysis can occur after ultimately involved in the production of reduced administration of any of the above drugs medications ranitidine best buy for cabgolin. Medical disorders and anaesthetic problems G However symptoms 9 days post ovulation buy 0.5 mg cabgolin with visa, haemolysis has occurred sodium nitroprusside or prilocaine (Smith & intraoperatively in the absence of these drugs Snowdon 1987 symptoms 11dpo generic 0.5 mg cabgolin otc, Martin & Casella 1991). Infants are more susceptible to oxidative stress than adults (Martin & Casella 1991). The SpO2 was 86%, but on Intraoperative hemolysis:the initial manifestation of blood gases oxygen levels were normal. Younker D,DeVore M,Hartlage P 1984 Malignant hyperthermia and glucose-6-phosphate Management dehydrogenase deciency. Elective surgery should not be undertaken during a haemolytic episode, or in the presence of an infection. The Casson H 1975 Anaesthesia for portacaval bypass in current classication is: patients with metabolic disease. Phenotypic,genetic,and the commonest of the diseases are dealt with biochemical characteristics,and therapy. Glycogen 0, which is not on the original Cori classication, is secondary to a deciency of glycogen synthase activity in the liver. Two postprandial hyperglycaemia and hyperlactic criteria are required for a diagnosis; an eye acidaemia (Wolfsdorf et al 1999). Medical disorders and anaesthetic problems G Preoperative abnormalities plethysmography and pulse oximetry before surgery, to assess the patency of the upper airway 1. Results did not suggest the the eyelid, epibulbar dermoid, subconjunctival presence of severe obstruction, therefore lipoma, and defects of the extraocular muscles. Cervical anomalies and basilar impression using a guidewire or a mask adaptor (Okuyama can occur (Gosain et al 1994, Manaligod et al et al 1994). Radiographic evidence of fusion of the cervical vertebrae was present in 11 out of 18 3. Management of a neonate with transposition of the great vessels and hydrocephalus has been 5. Aoe T,Kohchi T,Mizuguchi T 1990 Respiratory inductance plethysmography and pulse oximetry in 6. Bahk J-H,Han S-M,Kim S-D 1999 Management of difcult airways with a laryngeal mask airway under propofol anaesthesia. A retrospective study of seventeen distress underwent respiratory inductance cases. Cervical vertebral anomalies in patients with Lung function tests show a restrictive type of anomalies of the head and neck. Okuyama M,Imai M,Fujisawa E et al 1994 [Fiberscopic intubation under general anesthesia for 4. Pulmonary haemorrhage that may, on 212 occasions, be life-threatening (Klasa et al 1988). Impaired renal function and sometimes A rapidly progressive syndrome of renal failure. Plasma exchange may reduce cross-react with alveolar basement membrane, levels of plasma cholinesterase. Management the term is often applied more loosely, to any disease with pulmonary haemorrhage and 1. Elective antibodies are present (Holdsworth et al 1985, pulmonary surgery should not be undertaken Lee & Marks 1999). Assessment of renal function and haemorrhage and renal failure, but without the appropriate management. The management of a successful pregnancy has been described (Yankowitz et al Preoperative abnormalities 1992). Usually presents with cough, dyspnoea, steroids was associated with hyperglycaemia, haemoptysis (that can be massive), and anaemia. Problems of reduction in lung function in the presence of an effusion or a chylothorax (McNeil et al 1996). Complications associated with A nonmalignant, but sometimes fatal, syndrome malnutrition from loss of protein from the of massive osteolysis complicated by chylothorax; one patient was draining lymphangiomatosis. A Anaesthesia was reported for revision of mass of proliferating, thin-walled vascular and pleurosubclavian shunt (Mangar et al 1994). The process often begins effusions following spinal decompression (Szabo after minor trauma. Mandibular and maxillary involvement Although grafting can be performed, resorption (Ohya et al 1990). In one patient, massive mandibular osteolysis resulted in obstructive Preoperative abnormalities sleep apnoea syndrome (Kayada et al 1995). Osteolysis; areas most commonly affected Bone grafts may subsequently undergo are the shoulder, upper arm, pelvis, jaw, thorax, resorption. Riantawan P,Tansupasawasdikul S,Subhannachart P 1996 Bilateral chylothorax complicating massive 2. A collective name given to a group of acute ascending polyneuropathies in which motor Bibliography involvement predominates. Characteristic electrodiagnostic features Preoperative abnormalities may be present. Muscle weakness usually starts in the legs, is symmetrical, and progresses upwards at a Anaesthetic problems variable rate. This progressive weakness, together with areexia, are required for the diagnosis. If the intercostal muscles are affected, Cranial nerve involvement, usually of the bulbar respiration and sputum clearance may be and facial nerves, may occur in up to 50% of compromised. Bulbar weakness may result in cases, although involvement of other nerves has pulmonary aspiration and segmental collapse. Autonomic dysfunction can produce cord paralysis was the rst sign (Panosian & postural variations in blood pressure and Quatela 1993). In some cases there is respiratory profound hypotension on induction of insufciency and an inability to clear secretions. Mild paraesthesiae in the toes and to be caused by a combination of hypotension ngertips may precede the muscle weakness. Pain may be a troublesome feature and is muscular pain with tenderness, and burning or difcult to treat. Autonomic dysfunction may produce associated with transient severe hyperkalaemia cardiovascular instability and an impairment of and cardiac arrest (Dalman &Verhagen 1994). It has been suggested that the lack of respiratory variation in heart rate, which is 6. Cardiac arrest difference in outcome (van der Meche et al after suxamethonium was reported in a pregnant 1992,Winer 1992,Anonymous 1997). Weakness following general anaesthesia occurred in a patient who failed to disclose a 4. Constipation should through an epidural catheter for postoperative be anticipated, with the use of stool pain relief. The use of accessory muscles of treatment of intractable pain (Connelly et al respiration, and the reduction of vital capacity to 1990). The use of esmolol in its cardiac output, beta adrenoceptor blockade may management. Medical disorders and anaesthetic problems H Haemoglobinopathies (sickle cell Sickle cell disease disease) (see also Thalassaemia) A genetic abnormality of haemoglobin synthesis Normal haemoglobin (HbA) consists of a involving the substitution of valine for glutamic colourless protein, globin, which is made up acid at the sixth amino acid position in the beta from two alpha and two beta polypeptide chains, chain of the globin molecule. The haem radical is a frequently in blacks of African origin and in porphyrin structure, at the centre of which is a some Mediterranean races. Haemoglobinopathies associated with cell membrane is deformed by these molecular unstable haemoglobin. The process is complex and the precise mechanism of vaso occlusion is not known (Steinberg 1999). Sickle cell disease is associated with small Cooperative Study of Sickle Cell Disease and vessel occlusion and episodes of infarction in the Preoperative Transfusion in Sickle Cell affected organs. Reduced oxygen tension and al 1994), morbidity and mortality associated with acidosis cause sickling of red cells. The surgery and anaesthesia (Koshy et al 1995), and a 219 increased viscosity encourages stasis and trial of preoperative aggressive transfusion versus sludging, which in turn produces occlusion, conservative transfusion (Vichinksy et al 1995, ischaemia, and infarction. Papillary necrosis and haematuria Acute pain teams are increasingly being involved can develop as a result of sickling in the in the management of painful sickle cell crises. For elective procedures,the genotype should massive sudden pooling of red cells, be determined by haemoglobin electrophoresis. Medical disorders and anaesthetic problems H d) Haemolytic crises sometimes occur in marrow transplantation (Steinberg 1999). At association with glucose-6-phosphate present, the benets have to be weighed against dehydrogenase deciency following drug the possible complications (Cohen 1998). Infants less than 6 months old have high Anaesthetic problems percentages of HbF, therefore may not require transfusion. Sickling of red blood cells may be precipitated by hypoxia, acidosis, cold, and 8. Organ infarction, ischaemia, and recurrent episodes of chest pain, fever, with the further hypoxia, may result. An alternative progressive decreases in the saturation of theory is that rib infarction causes pleuritis and haemoglobin with oxygen. Despite statements techniques showed that these changes are further to the contrary, anaesthetics in those with sickle accentuated in a sickle cell crisis, possibly as a cell trait have not been entirely free from result of shunting (Singer et al 1989). Superior sagittal sinus thrombosis infarcts, have been reported in 17% of young occurred in a child following eye surgery (Dalal patients with sickle cell disease (Kinney et al et al 1974). Cholelithiasis is common, and reported and subsequent maternal death occurred during incidences vary from 4% to 55%, depending on Caesarean section (Anaesthetic Advisory the method of diagnosis. Laparoscopic Committee to the Chief Coroner of Ontario techniques are becoming common (Ware et al 1987). In one patient, conversion to open hypoxic, acidotic and sickled blood to the heart.
Desde el punto de vista histologico se clasifican en: capilares treatment improvement protocol cheap 0.5mg cabgolin with visa, venosas medications bipolar disorder purchase cabgolin 0.5mg amex, arteriovenosas symptoms detached retina buy cabgolin 0.5mg with amex, linfaticas y mixtas o combinadas treatment toenail fungus buy generic cabgolin online. Desde un punto de vista clinico se clasifican en malformaciones de alto y bajo flujo treatment 001 - b order cabgolin online from canada. Las que tienen componente arterial se consideran de alto flujo y las que carecen de dicho componente son consideradas de bajo flujo medicine x ed cheap cabgolin 0.5mg with amex. Nevus anemico Malformacion poco comun de tipo funcional, ya que anatomicamente los vasos son normales. Es debida a una reactividad aumentada de los vasos a las catecolaminas, que provoca una vasoconstriccion permanente. Clinicamente consiste en una macula blanquecina de margenes irregulares y frecuentemente acompanada de lesiones satelites. Es mas frecuente en el sexo femenino y puede aparecer en cualquier localizacion, aunque la parte superior del tronco es la mas comun. Al friccionar energicamente la lesion, esta permanece blanca y la zona periferica se enrojece (a diferencia de los nevus acromicos, que si se enrojecen al friccionarlos). El examen con luz de Wood no acentua la lesion, al contrario de lo que ocurre con las lesiones debidas a falta de melanina. Cutis marmorata telangiectasica congenita Esta malformacion se caracteriza clinicamente por maculas de color rojo-violaceo que se disponen formando un reticulado que recuerda el veteado del marmol, de ahi su nombre 12-4. Nevus flameo o mancha en vino de Oporto El nevus flameo, llamado tambien angioma plano (nombre inadecuado ya que se trata de una malformacion), se presenta en forma de maculas de color rosado que pueden aparecer en cualquier parte del cuerpo, aunque la cara es la localizacion mas frecuente 12-5. Las manchas, con la edad, toman un color rojo mas intenso y terminan de color violaceo. Cuando afecta a la cara hay que descartar un glaucoma, el 10% de los nevus flameos faciales pueden presentar esta complicacion, especialmente frecuente si se afecta el territorio de las ramas oftalmica y maxilar del trigemino. Otra posible asociacion es el sindrome de Klippel-Trenaunay 12-6, que consiste en el aumento de tamano de un miembro (con o sin hipertrofia osea). El sindrome de Sturge-Weber consiste en la presencia de un nevus flameo facial generalmente extenso que afecta la frente, zona periocular y area maxilar. Aunque la lesion suele ser unilateral, un 50% pueden presentar afectacion bilateral de la cara 12-7. El sindrome tambien presenta afectacion vascular leptomeningea y en un 30-60% afectacion ocular. Las manifestaciones neurologicas mas comunes son epilepsia y retraso mental, aunque tambien pueden presentarse hemiplejia, hemianopsia y defectos sensoriales. El tratamiento de la mancha en vino de Oporto se realiza con laseres vasculares como el de colorante pulsado (Candela) o el neodimio-yag (Vascu-light), o mediante luz intensa pulsada (Photoderm). Los resultados son mejores si el tratamiento se realiza en la infancia que si se espera a la edad adulta. Mancha salmon Se trata de una lesion macular de color rojo claro (salmon) que se localiza en los parpados, region glabelar y nuca. Es muy frecuente, afectando al 25-40% de los recien nacidos y tiende a desaparecer durante los primeros anos de vida. La mancha salmon localizada en la nuca (conocida coloquialmente como picadura de la ciguena), suele ser mas persistente y a menudo se mantiene durante la edad adulta. Marcas vasculares hiperqueratosicas Patologia poco frecuente a la que tambien se ha denominado hemangioma verrucoso, y aun se emplea este termino, pero es inadecuado ya que se trata de una verdadera malformacion y no de un hemangioma (neoplasia). Se trata de placas de color rojo purpura o azulado, que crecen lentamente y van desarrollando una franca hiperqueratosis en su superficie que les dan un aspecto verrucoso 12-8. El tratamiento es dificil y la unica opcion es la cirugia cuando las lesiones no son de gran tamano. Malformaciones venosas Las malformaciones venosas han sido a menudo mal llamadas hemangiomas cavernosos. Estan siempre presentes en el nacimiento y aumentan de tamano proporcionalmente al crecimiento del nino. No involucionan y, por tanto, siempre van a estar presentes a lo largo de la vida del paciente. Tambien se pueden encontrar flebolitos calcificados en el interior de las mismas y pueden ocurrir episodios de tromboflebitis en las lesiones o en su proximidad. Suelen ser asintomaticas, pero pueden provocar defectos esteticos y compresion de estructuras vecinas. Las malformaciones venosas pueden asociarse a otras anomalias y formar parte de sindromes mas complejos 12-10. Puede ser heredado de forma autonomica dominante, aunque existen casos esporadicos. Se trata de nodulos azulados facilmente compresibles, generalmente de pequeno tamano y que recuerdan a la presion a la tetina de un chupete. En la piel suelen existir pocas lesiones, pero en el tracto intestinal son a menudo multiples y es frecuente el sangrado espontaneo, lo que provoca melenas y anemia. Aunque es menos frecuente, tambien pueden existir estas malformaciones venosas en otros organos como pulmon, corazon, higado, cerebro. Si la clinica de melenas y anemia es recurrente estaria indicada la reseccion del segmento intestinal afecto. Sindrome de Maffucci Se caracteriza por malformaciones venosas, encondromatosis asimetrica difusa y deformidades esqueleticas. Al nacimiento no suelen ser visibles las malformaciones, poniendose de manifiesto las lesiones en la primera infancia. Se trata de nodulos o tumores de color azulado que suelen afectar mas a las extremidades. A esto se asocian tumores oseos de los huesos largos, manos y pies, que corresponden a encondromas, y pueden provocar importantes deformidades 12-11. En un 15% de los pacientes estos tumores pueden degenerar y desarrollar un condrosarcoma. Malformaciones linfaticas La clasificacion de los distintos tipos de malformaciones linfaticas se detalla en 12-12. Malformaciones linfaticas microquisticas o superficiales Estas malformaciones, mal llamadas linfangioma circunscrito (ya que no se trata de un tumor), suelen presentarse en el nacimiento o primera infancia. Pueden localizarse en cualquier area anatomica, pero las axilas, zonas proximales de las extremidades y la lengua son los sitios de eleccion. Clinicamente, se caracterizan por multiples lesiones de aspecto similar a vesiculas agrupadas en placas, a modo de huevos de rana. En ocasiones presentan un componente de vasos sanguineos asociado que hace que algunas lesiones tengan color rojo 12-13. El tratamiento es quirurgico, pero son frecuentes las recidivas ya que es dificil establecer los limites de la lesion y a veces existe un componente profundo de la malformacion que favorece las recurrencias. Suelen ser asintomaticas, pero producen importantes deformidades esteticas 12-14, y ocasionalmente comprometen la respiracion o la alimentacion, al comprimir la via aereodigestiva alta. No suelen estar presentes al nacimiento y si lo hacen (40%) es en forma de una mancha eritematosa de pequeno tamano. En las primeras semanas de vida crecen rapidamente para despues en la mayoria de los casos involucionar. Existen distintos tipos de hemangiomas que se resenan en 12-15, pero hablaremos fundamentalmente de los mas frecuentes en la infancia (hemangioma infantil) y de aquellos que puedan provocar problemas o complicaciones en el nino (angioma en penacho y hemangioendotelioma kaposiforme). Historia natural Los hemangiomas infantiles tienen una primera fase proliferativa en la que crecen y que acontece en el primer ano de vida y otra fase involutiva que dura varios anos. En el 40% de los casos el hemangioma esta presente al nacimiento y puede evidenciarse algun signo del mismo, en forma de macula telangiectasica, lesion equimotica o macula equimotica con halo palido. La mayoria de los casos inician su fase de crecimiento en las primeras semanas de vida, aunque algunos hemangiomas mas profundos pueden no detectarse hasta pasados varios meses. Esta fase de crecimiento rapido puede ser mas intensa durante los primeros 3 a 6 meses y la mayoria de estos tumores terminan su crecimiento entre los 9 y 12 meses de edad. Un pequeno porcentaje de hemangiomas apenas sufre cambios desde el nacimiento y otra pequena minoria continuaran creciendo durante mas de un ano. La fase involutiva se produce a partir del primer ano de vida y el hemangioma sustituye el componente vascular por tejido fibroadiposo, por lo que pierde en parte su color rojo, aparecen areas o bandas blanquecinas y se hace mas blando. La involucion completa se observa con una frecuencia aproximada de un 10% por ano, por lo que un 50% involuciona a los 5 anos, un 70% a los 7 y un 90% a los 9 anos. Al involucionar pueden quedar secuelas, a veces minimas como telangiectasias o piel atrofica, y en ocasiones cambios mas significativos como piel redundante con residuos fibroadiposos y cicatrices especialmente si el angioma se ulcero. A medida que involucionan, las luces vasculares se dilatan, las celulas endoteliales se aplanan y se deposita tejido fibroso, dando al hemangioma una arquitectura lobular. Clinica El aspecto clinico de los hemangiomas varia dependiendo de la localizacion del tumor, de ahi que se clasifiquen en hemangiomas superficiales, profundos y mixtos. Los superficiales asientan en la dermis superficial y son de color rojo brillante, por eso se las llama hemangiomas en fresa 12-16. Los hemangiomas profundos se desarrollan en la dermis reticular y tejido celular subcutaneo, y se manifiestan como masas blandas de tonalidad azulada o del color de la piel 12-17. Los hemangiomas infantiles pueden localizarse en cualquier zona del cuerpo, dandose con mas frecuencia (60%) en cabeza y cuello. Desde el punto de vista del area que afectan tambien se clasifican en focales, cuando afectan a una zona pequena, o en segmentarios (similares a placas) cuando afectan a un segmento anatomico mas amplio 12-18. Estos ultimos suelen asociarse con mayor frecuencia a complicaciones, como veremos mas adelante. Complicaciones El 10% de los hemangiomas presentan complicaciones que pueden ser debidas al propio tumor o bien derivadas de su localizacion. Habitualmente se produce durante la fase proliferativa y suele ocurrir en hemangiomas situados en zonas de friccion o maceracion, como la boca y el area anogenital. Las ulceraciones son dolorosas y por eso si se localizan en los labios pueden dificultar la alimentacion y en la zona anogenital la defecacion o miccion. Se caracterizan por la presencia de un exudado purulento y aumento del calor y el dolor. Se deben realizar cultivos del exudado y tratar la infeccion con antibioticos por via topica y sistemica. Suele ser un sangrado leve o moderado en angiomas ulcerados y que se resuelve facilmente con compresion directa. Mas raro es una hemorragia profusa que puede ocurrir por un fenomeno de Kasabach-Merritt (coagulopatia de consumo), lo cual es muy raro en hemangiomas infantiles clasicos, siendo mas comun en hemangioendoteliomas kaposiformes y angiomas en penacho. Estas secuelas pueden ocurrir con la propia involucion del tumor y son mas frecuentes en aquellos de gran tamano. Complicaciones debidas a la localizacion del hemangioma Como comentabamos los hemangiomas segmentarios de ciertas localizaciones pueden dar lugar a ciertas complicaciones 12-21, que describimos a continuacion. Esta presentacion requiere un control y estudio muy estricto ya que pueden provocar importantes problemas. La complicacion mas importante es la ambliopia o vision reducida del ojo afecto, debida a la deprivacion de estimulo visual en los hemangiomas que por su tamano obstruyen el eje visual. Otra complicacion frecuente es la deformacion de la cornea inducida por la presion local directa del tumor, lo cual provoca astigmatismo. Estos tumores pueden provocar obstruccion de la via aerea superior y provocar sintomas de tos, disfonia e insuficiencia respiratoria, por lo que precisan de un estudio otorrinolaringologico detallado. La presencia de un hemangioma en region lumbosacra debe alertar sobre la posibilidad de un disrafismo espinal oculto o de alteraciones genitourinarias. El termino hemangiomatosis se utiliza para describir la presencia de hemangiomas generalizados de pequeno tamano, pudiendo existir entre pocos elementos y centenares. Puede existir solo afectacion cutanea, utilizandose el termino hemangiomatosis neonatal benigna, pero puede haber afectacion visceral, especialmente afectacion hepatica, en este caso se utiliza el termino de hemangiomatosis neonatal diseminada. La afectacion hepatica puede representar un mal pronostico y estos casos deben ser tratados con corticoides sistemicos. Tratamiento La mayoria de los hemangiomas no requieren tratamiento, ya que involucionan espontaneamente. No existen unos criterios protocolizados de tratamiento, debiendose valorar cada caso individualmente. Los corticoides sistemicos son la primera herramienta en el tratamiento de los hemangiomas. La dosis recomendada es generalmente de entre 2 y 3 mg/kg de prednisona en una dosis unica matinal. El tratamiento se realiza de 4 a 6 semanas y luego se reduce gradualmente la dosificacion. Se deben utilizar en la fase proliferativa, que es cuando se consiguen mejores resultados. Los efectos secundarios mas frecuentes son fiebre y sindrome seudogripal que pueden tratarse con paracetamol. Por ello, hoy dia se recomienda usar este farmaco solo en casos de angiomas con complicaciones graves que no han respondido a esteroides. Se emplea en hemangiomas de gran tamano y en casos asociados a fenomeno de Kasabach-Merritt. La dosis habitual es de 0,05 mg/kg en ninos menores de 10 kg o 1,5 mg/kg en ninos con peso superior a 10 kg, administrados via intravenosa de forma semanal. Esta indicado en las telangiectasias residuales que pueden permanecer tras la involucion. Tambien se ha utilizado en los hemangiomas ulcerados y, aunque es un tema controvertido, algunos autores lo utilizan en angiomas de pequeno grosor durante la fase proliferativa. Puede estar indicada en hemangiomas de los parpados que no responden a tratamiento medico. Se emplearia en hemangiomas hepaticos con fistulas arteriovenosas, que suelen provocar insuficiencia cardiaca. Tambien existen casos de aparicion en el nacimiento y en la edad adulta, Suele localizarse en el cuello, hombros y zona alta del tronco, aunque puede aparecer en otras zonas del cuerpo. El aspecto clinico es muy variable, puede presentarse en forma de macula, placa o nodulo 12-24.
Lesions of the orbi formed by the limbic system of the brain symptoms queasy stomach buy cabgolin without a prescription, which tofrontal cortex produce disinhibited behaviors that includes the cingulate cortex symptoms for mono buy line cabgolin, amygdala treatment 32 for bad breath purchase cabgolin mastercard, thalamus medications lexapro 0.5mg cabgolin, may transgress accepted social norms medicine keri hilson lyrics cabgolin 0.5mg visa. Perrier Memory Center of an academic hospital for progres activities autonomously medications given during dialysis cheap 0.5mg cabgolin. His past medical history in tation progressed until he ultimately got lost in the C. There was no family history of any psychiat he began making sexually inappropriate comments that ric or neurologic disorders. Karl sentation with memory loss and word-finding difficul mission revealed a severe amnestic syndrome, dif Mondon, Centre Memoire de Ressources et de Recherche, ties. Six months later, his wife observed a progressive ficulties in naming and verbal comprehension, Hopital Bretonneau, 2 Bd loss of interest in his previous hobbies and increasing visuospatial impairment, a cognitive and behav Tonnelle, 37044 Tours, Cedex, France apathy. Twelve months after symptom onset, the pa ioral prefrontal syndrome, and multimodal visual karl. At the same time, his wife observed a personal neurologic examination was normal. First, potentially curable causes of dementia When pyramidal, cerebellar, or choreiform movements should be excluded. Motor im pugilistica), or inflammatory (multiple sclerosis) le pairment or a concurrent movement disorder suggests sions. Laboratory tests assess the most frequent endo subcortical causes of dementia such as Parkinson disease crine and metabolic disorders (thyroid, parathyroid, dementia, progressive supranuclear palsy, and cortico B12, thiamine, folate and niacin deficiencies, hypo basal degeneration. Finally, global (Alzheimer disease) glycemia, hepatic encephalopathy, renal failure). Laboratory tests of with a widespread increase in theta activity, predom the adrenal and pituitary functions could be per inately in the temporal regions. Metabolic studies can assess for leukodystro bilateral temporal lobe atrophy, markedly more se phies, encephalopathies, and porphyria. If sleep vere on the right side (figure), while the other cortical apnea is suspected, polysomnography can be under regions, including the frontal lobes, were normal. If imaging suggests normal pressure hydro There were no white matter abnormalities. Question for consideration: If the evaluation remains inconclusive, degenerative etiologies should be considered. International Classification of Diseases and Health Related Problems, 10th Revision. Geneva: World Health Organi dromes, which can be divided into 3 groups: 1) zation; 1992. Frequency and 7 clinical characteristics of early-onset dementia in consecu tia lacking distinctive histopathology. The accurate diagnosis of early-onset demen long time, prosopagnosia was considered the main tia. Frontotemporal Thus, the right temporal variant of frontotemporal lobar degeneration: a consensus on clinical diagnostic cri lobar degeneration can be considered to be the right teria. Frontotemporal dementia and related disor Recently, investigators delineated the cognitive pro ders: deciphering the enigma. Questions for consideration: On the day prior to presentation, the patient began having memory difficulties and was noted by her 1. What is the differential diagnosis for subacute Correspondence to husband to have completely forgotten many events memory disturbances and confusion in this Dr. Infectious workup was notable for a rapid confusion or exposure to psychoactive medications influenza swab that was positive for influenza A. Finally, transient Questions for consideration: global amnesia is a consideration, but is a diagnosis of exclusion. What is the differential diagnosis of subacute intracranial imaging to assess for mass lesion, altered mental status and seizures in association stroke, or hemorrhage. Reflexes were brisk, measuring 3/4 in all abnormalities; thus, the seizures should be viewed as 4 extremities, and the patient had positive Hoffman symptomatic of another pathologic process until signs, flexor plantar response on the right, and equiv proven otherwise. How do you interpret the results of lumbar the patient was treated with acyclovir and levetira puncture On enza, and Cryptococcus as well as testing for enterovi follow-up 8 months later, the patient was fully ambu ruses or arboviruses depending on the season. Repeat lumbar puncture in the mesial temporal lobes and thalami consistent showed total protein of 794 mg/dL, glucose of with necrotizing encephalitis. Additional extensive 84 mg/dL, with 4 leukocytes and 19 erythrocytes workup for infectious encephalitis was negative. Chest X-ray demonstrated a association with symmetric hemorrhagic brain left lower lobe opacity, and the patient was treated lesions. Jenelle Acute hemorrhagic leukoencephalopathy associated with Jindal cared for the patient and helped in discussion of the manuscript. She recalled 2 of 3 words at 5 minutes, but had no mem presented to the obstetrical service fully dilated af ory for recent events, including her delivery. She ter 2 days of leaking vaginal fluid, and delivered a could not describe cocktail ingredients, despite work Address correspondence and healthy baby girl. A few hours later, she did not ing as a bartender, but correctly recited old addresses. Grinspan, Division of Pediatric Neurology, Harkness neurology service for evaluation. Pavilion, 5th Floor, 180 Fort She had had a febrile seizure at age 4, and several Strength was full. She had 2 healthy Questions for consideration: children, 1 abruption at 23 weeks, and 1 elective 1. Subacute processes, such as de onset encephalopathy with memory loss and abulia, myelinating diseases and paraneoplastic processes, as well as long tract signs. Focal insults to Serum chemistries were normal except for low total structures responsible for memory or attention, such protein (5. Lumbar puncture re the differential diagnosis includes emergent vealed a protein of 121 mg/dL, normal glucose, 3 white peripartum conditions, such as dural sinus throm 3 3 blood cells/mm, and 23 red blood cells/mm. Urine bosis, metastatic choriocarcinoma, and postpar tum angiopathy, a form of reversible cerebral toxicology was positive for marijuana. Neurology 73 October 13, 2009 e7513 agulation, endocrine, cardiac, lipid, and immunologic caliber changes in the distal branches of both middle studies were unrevealing. Subtle memory problems had be hypointense on T1-weighted imaging and some gun 1 month prior. There were multi Questions for consideration: ple lesions in the corpus callosum, many with a rim of T2 hyperintensity around a center of T1 hypoin 1. What further testing would help distinguish among these worsens over hours to days, and lasts days to weeks, diagnoses Digital tance of the history in an encephalopathic patient and subtraction angiography found generalized small cal the utility of a broad differential diagnosis. Bedside under 100 m in the cochlea, retina, and brain (rather dilated funduscopic examination revealed bilateral than muscle and skin, as in dermatomyositis). The current literature only describes about 100 pa Muscle biopsy and additional serum tests to look for tients with Susac syndrome, but the disease is underap evidence of endothelial damage were obtained. Women dothelial antibody tests were weakly positive, and factor outnumber men 3:1. Months to years may separate the initial symp cells, and may rise if they are damaged. We diagnosed Susac syndrome, or retinocochleo often migrainous, frequently precedes the onset of en cerebral vasculopathy, based on the pathognomonic cephalopathy, and progresses to confusion, memory loss, behavioral changes, dysarthria, and mutism. Only after an unrevealing evaluation for matter lesions in the cerebral hemispheres. Also of show restricted diffusion, suggesting they represent note, initial bedside funduscopic examination found small infarcts. The character tum, she demonstrated right visual field deficits, brisk istic callosal lesions in Susac syndrome are frequently reflexes, and clonus at both ankles, right more than left. She fatigues easily, but manages household chores size of the affected arterioles is below the resolution of and childcare on her own. Tullman has received research support from Acorda Ther sionally monocular amaurosis fugax. Post partum cerebral angiopathy: reversible vasoconstriction as Only 7 pregnancies in 6 patients with Susac syn sessed by transcranial Doppler ultrasounds. Retinocochleoce tion, and as many as 1/3 have relapse of encephalop rebral vasculopathy. Mycophenolate mofetil was added after weighted imaging and apparent diffusion coefficient val a week, as she had not significantly improved, and the dis ues. Fluorescein and Mycophenolate mofetil was chosen over cyclophospha indocyanine green angiographies in Susac syndrome. However, the patient improved clin of the brain and retina with hearing loss in young women. One Burns, Mayo Clinic, Department toothpaste on a toothbrush, which he described as of Neurology, 200 First Street week later, he suddenly became confused while driving. In addition to the childhood seizures, his past Over the next 2 weeks, he had several similar spells. He also developed recurrent, sudden, severe headaches that medical history was notable for a fungal infection of occurred several times per day. The pain began in the the lung in 1997 for which he had been admitted to shoulders, spreading to the occipital region and then the an intensive care unit. It was severe enough to not known beyond the fact that he was treated for cause him to fall to his knees and cry out in pain. He had a remote episodes occurred more frequently when lying in bed smoking history. What is the differential diagnosis for this clinical for evaluation of these symptoms and transferred to our presentation What features of the history are most useful in narrowing resolved spontaneously, while there. In this case, the history has two main compo right arm and little finger suggests a lesion of the nents: spells of altered consciousness and episodes of ulnar nerve or C8 root, while the knee buckling may severe headache. The localize to the femoral nerve, lumbar roots, thoracic spells of altered consciousness are most consistent spinal cord, or medial left frontal lobe. The sudden, severe ther semiologic characterization, the dysarthria could headaches have a broader differential diagnosis, in localize to a number of structures and therefore is of cluding venous sinus thrombosis, posterior reversible little localizing value. He was thin and appeared chron A history of multiple recurrences without severe neu ically ill. The remainder rologic sequelae argues strongly against subarachnoid of the general medical examination was unremark hemorrhage and cervical artery dissection. On neurologic examination, he was listless, is unlikely in light of the sudden onset, postural vari somewhat inattentive, and seemed unconcerned with ations, and associated intermittent confusion. The cranial nerves were normal and there sodic intracranial hypertension from a mass lesion, hydrocephalus, meningitis, or some combination of was no papilledema. Motor examination revealed a these diagnoses is an important consideration given right pronator drift and a low-amplitude, high the positional nature of the headaches. Muscle stretch Equally crucial to formulating a neurologic differ reflexes were normal with the exception of brisk knee ential diagnosis is to begin to localize the disease pro reflexes. Plantar responses were equivocal on the cess within the nervous system from the history. Pinprick sensation was Doing so allows one to narrow the list of possible reduced on the medial aspect of the right hand, in etiologies. Complex par vibration as well as cortical sensory function were tial seizures localize to the frontal or temporal lobe. While the long duration of the event and the postic Questions for consideration: tal period suggests a temporal lobe focus, it is impos 1. Based on the history and examination, what is your clini sible to precisely localize the seizure focus in this case cal formulation What diagnostic tests would be useful to test this gests dysfunction of anterior portions of the frontal hypothesis
Cheap cabgolin 0.5 mg free shipping. SHINee - Honesty Instrumental (Sherlock 4th mini Album).
References
- Ruggenenti P, et al. Preventing microalbuminuria in type 2 diabetes. N Engl J Med 2004;351:1941-1951.
- Roffi M, Sievert H, Gray WA, et al: Carotid artery stenting versus surgery: adequate comparisons? Lancet Neurol 9:339-341, 2010; author reply 341-332.
- Divry P, Rolland MO, Zabot MT, et al. Mevalonic kinase deficiency in 2 siblings. Society for the Study of Inborn Errors of Metabolism. Proceedings of the 29th Annual Symposium, London, Sept 1991: 146 (Abstr.). 17.
- Sonmez MG, Kozanhan B: Complete response to acupuncture therapy in female patients with refractory interstitial cystitis/bladder pain syndrome, Ginekol Pol 88(2):61n67, 2017.

