
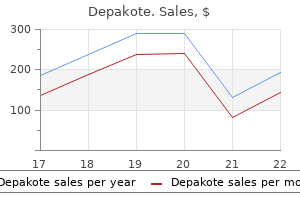
Steven P. Cohen, MD
- Assistant Professor
- Department of Anesthesiology
- John Hopkin School of Medicine and Walter Reed
- Army Medical Center
- Baltimore, Maryland
Some abnormalities evidenced in the fossilized limbs of these ancient populations could have been caused by recurring episodes of inadequate intake of ascorbic acid medications dialyzed out purchase depakote paypal. Future studies in paleopathology should bring additional interesting facts to light treatment 2 lung cancer generic 250mg depakote. Another way of assessing the extent of the ascorbic acid nutriture of these ancient peoples is to find out what current primitive societies used as food treatment nausea cheap 250 mg depakote fast delivery, and what their methods of food preparation and preservation were before "civilization" reached them: the Australian aborigine medications contraindicated in pregnancy buy generic depakote on line, the native tribes of Africa symptoms 3 days after embryo transfer discount depakote 250mg without a prescription, the Indians of the Americas medications joint pain buy 500mg depakote amex, and the Eskimo, who has worked out a pattern for survival in a most unfavorable environment. All products of the plant and animal kingdoms,without exception, were at one time or another consumer. Those who ate their food fresh and raw had more chance of 27 obtaining ascorbic acid. The name "Eskimo" comes from the Cree Indian work "uskipoo," meaning "he eats raw meat. Any Eskimo who cooked his fish and meat thereby reducing its ascorbic acid content would never have survived long enough to tell about his new-fangled technique of food preparation. The levels were, as always, greatly submarginal for optimal health and longevity, especially under high-stress conditions. The estimated life expectancy for an Eskimo man in northern Greenland is only twenty-five years. Two great advances in the early history of man were the development of agriculture and the domestication of animals. In the temperate zones, agriculture tended to concentrate on cereal grains or other seed crops, which could easily be stored without deterioration and used during the long winters. These crops are notably lacking in ascorbic acid and, while they supplied calories, scurvy would soon develop in those who depended on them as a staple diet. Whatever fresh vegetables or fruits were grown were generally rendered useless as an antiscorbutic foodstuff for winter use by the primitive methods of drying and preservation. A trick for imparting antiscorbutic qualities to seed crops was discovered by various agricultural peoples and then forgotten. It was rediscovered again in Germany in 1912, and it has persisted among some Asiatic people. This simple life saving measure was to take portions of these seed crops (beans and the like), soak them in water, and then allow them to germinate and sprout. Ascorbic acid is required by the growing plant and it is one of the first substances that is synthesized in the growing seed to nourish the plant embryo. Bean sprouts are even now a common item of the Chinese cuisine as they have been for thousands of years; but they contain our elusive molecule, while unsprouted beans do not. If they used these products fresh they were safe, but if they attempted long preservation, the antiscorbutic properties were lost and the foodstuffs became potential poisons. All in all, it has been a terrible struggle throughout prehistory and history to obtain the little daily speck of ascorbic acid required for mere survival. Before discussing this great scourge of mankind, let us examine the disease caused by this genetic defect. Clinical scurvy is such a loathsome and fatal affliction that it is difficult to conceive that an amount of ascorbic acid that could be piled upon the head of a pin is enough to prevent its fatal effects. In describing the disease we must distinguish between chronic scurvy and acute scurvy. It is a condition where the normal biochemical processes of the body are not functioning at optimal levels because of the lack of sufficient ascorbic acid. The chronic form usually exists without showing the clinical signs of the acute form and this makes it difficult to detect and diagnose without special biochemical testing procedures. The acute form is the "classical" scurvy recognized from ancient times and is due to prolonged deprivation of ascorbic acid, usually combined with severe stress. The first symptom of acute scurvy in an adult is a change in complexion: the color becomes sallow or muddy. There is a loss of accustomed vigor, increased lassitude, quick tiring, breathlessness, a marked disinclination for exertion, and a desire for sleep. Reddish spots (small hemorrhages) appear on the skin, especially on the legs at the sites of hair follicles. Sometimes there are nosebleeds or the eyelids 30 become swollen and purple or the urine contains blood. These signs progress steadily the complexion becomes dingy and brownish, the weakness increases, with the slightest exertion causing palpitation and breathlessness. The gums become spongier and bleed, the teeth become loose and may fall out, the jawbone starts to rot,and the breath is extremely foul. Old healed wounds and scars on the body may break open and fresh wounds and sores show no tendency to heal. The gums swell so much that they overlay and hide the teeth and may protrude from the mouth. The joints become so disorganized that a rattling noise can be heard from the bones grating against each other when the patient is moved. Death usually comes rapidly from sudden collapse at slight exertion or from a secondary infection, such as pneumonia. This sequence of events, from apparent health to death, may take only a few months. Acute clinical scurvy was recognized early by ancient physicians and was probably known long before the dawn of recorded history. Each year in the colder climes, as winter closed in, the populations were forced onto a diet of cereal grains and dried or salted meat or fish, all low in ascorbic acid. The consequence of this inadequate diet was that near the end of winter and in early spring, whole populations were becoming increasingly scorbutic. Thus weakened, their resistance low, people were easy prey for the rampant bacterial and viral infections that decimated the population. This happened year after year for centuries and this is the origin of the so-called "spring tonics," which were attempts to alleviate this annually recurring scurvy (by measures which were generally ineffective). The number of lives lost in this annual debacle and the toll in human misery are inestimable. People became so accustomed to this recurring catastrophe that it was looked upon as the normal course of events and casually accepted as such. Only in times of civil strife, of wars and sieges, or on long voyages, where the toll in lives lost to this dread disease was so great, did it merit special notice. The figure of the little man pointing to his mouth and the lips oozing blood indicated the bleeding gums of the disease. Sire Jean de Joinville, in his history of the invasion of Egypt by the Crusaders of Saint Louis in 1260, gives a detailed description of the scurvy that afflicted this army. He mentions the hemorrhagic spots, the fungous and putrid gums, and the legs being affected. It was scurvy that led to the ultimate defeat and capture of Saint Louis and his knights. It is certain that, throughout the Crusades, scurvy took a far greater toll of the Crusaders than all the weapons of the Saracens. In the great cycle of epidemics that hit Europe in the fourteenth century the Black Death of the Middle Ages millions of people died. The Black Death was a fulminating, virulent epidemic of a bacterial disease, bubonic plague, concurrent with pulmonary infection superimposed on scurvy with its diffused superficial hemorrhages that caused the skin to turn black or bluish-black. The fact that the disease attacked a population that was first thoroughly weakened by scurvy accounts for the extremely high mortality: one-fourth of the population of Europe or 25 million deaths. With the invention of the printing press and the easier dissemination of the printed word, the sixteenth and following centuries saw the appearance of many tracts that described scurvy and its bizarre causes, and offered many different exotic treatments and "cures" for the disease. Much earlier, folklore had associated scurvy with a lack of fresh foodstuffs, and the antiscorbutic qualities of many plants had been known. But these qualities were forgotten and had to be rediscovered again and again at a great cost in lives and suffering. Improved ship construction and the ensuing long voyages provided ideal conditions for the rapid development of acute scurvy under circumstances where the developing symptoms could be readily observed and recorded. Sailors quickly succumbed to scurvy due to inadequate diet; physical exertions; exposure to extremes of heat, cold, and dampness; and the generally unsanitary shipboard conditions. In a few short months, out of what started off as a seemingly healthy crew, only a few remained fit for duty and were able to stand watch. Before scurvy was finally controlled, this scourge destroyed more sailors than all other causes, including the extremely high tolls of naval warfare. In 1497, Vasco da Gama, while attempting to find a passage to the Indies by way of the Cape of Good Hope, lost 100 of his 160-man crew to scurvy. Three years later, only one ship, with only eighteen members of the original crew, returned to Spain. On occasion, a Spanish galleon would be found drifting, a derelict, its entire crew dead of scurvy. Many books were written on scurvy during the sixteenth to eighteenth centuries; some authors hit upon means to actually combat the disease, while others, clouded by the medical lore of the times, were way off base. We still find logs of eighteenth-century voyages that recount the devastating effects of scurvy, and others where the master of the ship was able to prevent the disease. In 1740, Commodore Anson left England with six vessels and 1500 seamen; he returned four years later with one ship and 335 men. Between 1772 and 1775, on his round-the-world trip, however, Captain James Cook lost only one man out of his crew of 118, and that one not from scurvy. Cook took every opportunity when touching land to obtain supplies of fresh vegetables and fruit. He usually had a good store of sauerkraut aboard and he knew the beneficial qualities of celery and scurvy grass. After the voyage was completed, Cook was 33 presented with the Copley Medal of the Royal Society. This award was given for his success in making such a lengthy voyage without a single death from scurvy not for his great navigational and geographic discoveries. This is only a very brief record of the easily avoidable havoc caused by scurvy on the high seas, but those on land fared little better. In addition to the fearful, annually recurring scorbutic devastation of the population in the late winter and early spring, there were special circumstances which brought on deadly epidemics of acute scurvy. In a brief sampling of the wars of the sixteenth to eighteenth century, scurvy appeared at the siege of Breda in Holland in 1625 and at Thorn in Prussia in 1703, where it accounted for 5,000 deaths among the garrison and noncombatants. It took its toll of the Russian armies in 1720 in the war between the Austrians and the Turks, of the English troops that captured Quebec in 1759, and of the French soldiers in the Alps in the spring of 1795. By the middle of the eighteenth century,the stage had been prepared for advances in the prevention and treatment of scurvy. Admiral Sir Richard Hawkins, in 1593, protected the crew of the Dainty with oranges and lemons; among others, Commodore Lancaster, in voyages for the East India Company, had shown by 1600 that scurvy was an easily preventable disease. Salisbury, was inspired by the hardships of the Anson fiasco and the many cases of scurvy he had treated on his own ships. Lind was a keen observer and eventually became known as "the father of nautical medicine. The crucial experiment Lind performed in 1747 at sea on the Salisbury, was to take twelve seamen suffering from the same degree of scurvy and divide them 34 into six groups of two each. In addition to their regular diet, he gave each group a different, commonly used treatment for scurvy and observed its action. One group received a quart of cider daily, the second group received twenty-five drops of dilute sulfuric acid three times a day, the third group was given two spoonfuls of vinegar three times a day, the fourth team drank half a pint of seawater three times a day, the fifth received a concoction of garlic, mustard seed, horseradish, gum myrrh, and balsam of Peru. These last two men improved with such astonishing rapidity that they were used as nurses to care for the others. There was slight improvement in the cider group but no benefit was observed in the others. Here was clear-cut, easily understandable evidence of the value of citrus fruit in the cure of scurvy. Although Lind did not realize it, he had found a good natural source of our elusive molecule. He continued his work on scurvy and, in 1753, published one of the classics of medical literature, A Treatise of the Scurvy. What as clear to Lind, and is commonplace to us, was not so readily accepted by the naval bureaucracy of his day. It has been estimated that this 42-year delay cost the Royal Navy 100,000 casualties to scurvy. This simple regimen wiped out scurvy in the naval forces of England, and it became their secret weapon for maintaining their mastery of the seas. There is no doubt that this simple ration of lemon juice was of far greater importance to the Royal Navy of the eighteenth and nineteenth centuries than all the improvements in speed, firepower, armor, and seaworthiness. Naval officers of the time asserted that it was equivalent to doubling the fighting force of the navy. Previously, because of the ravages of scurvy, the seagoing fleets had to be relieved every ten weeks by a freshly manned fleet of equal strength so that the scorbutic seamen could be brought home for rehabilitation. The impact of our elusive molecule on history has never been adequately evaluated. The English vessels were able to maintain continuous blockade duties, laying off the coast of France for months at a time without the necessity of relieving the men. Were it not for Lind, the flat-bottomed invasion barges assembled by Napoleon may well have crossed the English Channel. However, it takes much more than logic and clear-cut demonstrations to overcome the inertia and dogma of established thought. The British Board of Trade took 112 years until 1865 before similar precautions were adopted for the British merchant marine. There are records of seamen on the merchant vessels succumbing to scurvy even while delivering lemons to the ships of the Royal Navy. Over 30,000 cases of scurvy were reported in the American Civil War and it took the U. The saga of scurvy continues, with its incredible toll in human lives and suffering, up to the present day.
The parabasal cells of the overlying stratified gence of the tumour in the lymphocyte staining for high molecular weight cytok squamous epithelium symptoms rsv discount depakote 500 mg visa. There agnosis of Hodgkin or non-Hodgkin lym highlights the scanty wisps of cytoplasm are variable numbers of scattered S100 A B C treatment dry macular degeneration cheap 250 mg depakote otc. B Immunostaining for pan-cytokeratin highlights the surface epithelium as well and irregular clusters and sheets of positive cells (carcinoma) in the stroma symptoms flu purchase 500mg depakote amex. A Fine needle aspiration smear shows tight clusters of tumour cells among small lymphocytes treatment narcolepsy purchase depakote 250mg on-line. B In histological sections treatment 5th metatarsal shaft fracture cheap 500 mg depakote visa, examination under medium magnification often reveals areas where cohesive tumour growth is evident treatment urinary tract infection purchase 500 mg depakote fast delivery. C the epithelial nature of the tumour is readily confirmed by immunostaining for cytokeratin, whereby a meshwork pattern of staining is often observed. However, primitive or not evident in most cases of studies have reported the following fea since the diagnostic sensitivity of nasopharyngeal carcinoma at the light tures to be associated with a better prog nasopharyngeal cytology is limited (70 microscopic level, there is usually con nosis: high density of dendritic cells; high 90%) {387,1001}, nasopharyngeal biop vincing evidence of squamous differenti number of infiltrating lymphocytes; and sy is the preferred method for obtaining a ation at the ultrastructural level. At least low number of granzyme B-positive cyto definitive histological diagnosis . On the other hand, fine needle aspiration dles of tonofilaments or tonofibrils, in cytological examination of enlarged cer addition to well-formed desmosomes Epstein-Barr virus detection vical lymph nodes is invaluable in reach {1470, 1513,2082,2568}. The aspirate Crush artefacts are common in nasopha irrespective of the ethnic background of smears show, in a background of lym ryngeal biopsies, making it difficult to the patient. Such biopsies should be ing is often patchy and weak, and thus is cytoplasm of these cells is often fragile scrutinized in the better-preserved areas not a reliable method to demonstrate the and barely visible. A positive result also strongly suggests a nasopharyngeal origin (although not entirely specific) for a metastatic nonker atinizing carcinoma of unknown primary. B used in some centres to produce cyto Nasopharyngeal lymphoid hyperplasia mimicking nasopharyngeal carcinoma. In the left field, the venule logic preparations for diagnosis of with no obvious lumen can also be mistaken for a cluster of carcinoma cells. The presence of distinct by two subsequent negative biopsies mimic nonkeratinizing carcinoma. Clusters of germinal centre cells may be of cells, lack of large nucleoli, and nega Radiation-induced changes in the nor mistaken for carcinoma because of the tive staining for cytokeratin would be mal nasopharyngeal mucosa can be presence of large cells with vesicular against the diagnosis of carcinoma. The surface or nuclei and the absence of a well-defined Distinction between nonkeratinizing car crypt epithelium can exhibit enlarged, mantle zone. The identification of cinoma and large cell lymphoma can at hyperchromatic or even bizarre nuclei, admixed centrocytes (smaller atypical times be difficult. In the nasopharyngeal but such changes can be recognized to cells with irregular-shaped or angulated mucosa or metastatic deposit in lymph be benign because they are limited to nuclei) and tingible-body macrophages node, dispersed growth of the carcinoma some but not all cells (random cytologic points toward the lymphoid nature of the cells and accompanying eosinophil infil atypia) and the normal nuclear-cytoplas large cells, which can be confirmed by tration may lead to a misdiagnosis of mic ratio is maintained. Mucosal epithe immunostaining (leucocyte common anti Hodgkin lymphoma {330,394,2880}. These cells can be distinguished a diagnosis of nasopharyngeal carcino some foci a component of typical from residual or recurrent carcinoma by ma most unlikely . In con After treatment by radiation therapy, it nent endothelial cells and abundant fibri trast to the latter, the large cells are non may take weeks (up to 10 weeks) for the noid deposits. The can be confirmed by a lack of cytokeratin noma cells usually show evidence of nasopharyngeal biopsies should be immunoreactivity as well as positive radiation injury in the form of enlarged interpreted in the same way as for immunostaining for lymphoid markers in and bizarre nuclei, accompanied by an patients without a prior history of the large cells . Some recurrences, especial ly those occurring after a long interval (>5 years), may represent new primaries rather than a genuine relapse of the orig inal tumours . Radiation-induced tumours in the nasopharynx typically develop after a long latency period, and usually take the form of keratinizing squamous cell carcinomas or sarcomas (especially osteosarcomas) {403,600}. Keratinizing squamous cell carcinoma Histopathology this is an invasive carcinoma showing obvious squamous differentiation at the light microscopic level, in the form of intercellular bridges and/or keratinization over most of the tumour, morphologically similar to keratinizing squamous cell car cinomas occurring in other head and neck mucosal sites . The basaloid tumour cells show a fes as: well differentiated (most common), tooning growth pattern, and are interspersed by tumour cells with squamous differentiation. The tumour typically grows in the form of irregular islands, accompa ing carcinoma {1122,1859,2136,2318}, surround the individual tumour islands), nied by an abundant desmoplastic stro others have not found this subtype to dif but not in the cells showing obvious ma infiltrated by variable numbers of lym fer in biological behaviour {363,778}. The tumour cells are Immunoprofile and Epstein-Barr virus atinizing squamous cell carcinoma polygonal and stratified. The cells in the centres of the shows immunoreactivity for pan-cytoker Differential diagnosis islands or facing the surface often show atin, high molecular-weight cytokeratin, the frank invasive growth, nuclear atypia a greater amount of eosinophilic glassy and focally epithelial membrane antigen. In general, the patients have lower or geal carcinoma, distinction between a from mild to marked. To arrive at a definitive diagnosis, for locally advanced tumour growth (76% 580,599,961,1124,1125,1157,1176,1262 sometimes multiple biopsies are required versus 55%) and a lower propen,1885,1892,1988,2894}. Keratinizing to identify convincing stromal invasion as sity for lymph node metastasis (29% ver squamous cell carcinomas tend to carry well as focal mild nuclear atypia. A the surface epithelium consists of disarrayed cells with enlarged and crowded nuclei which vary in size, com patible with carcinoma in-situ. This patient was not given any treatment, and has remained disease-free at 7 years. C In this unusual example, the cells that comprise the surface epithelium exhibit marked nuclear pleomorphism and hyper chromasia. This example of radiation-associated carcinoma-in-situ has subsequently evolved into an invasive keratinizing squamous cell carcinoma. Sometimes there chapter on hypophyarnx, larynx and tra nent is identified in only 3-8% of cases, can be scattered amyloid globules. Four cases had stage T3 or T4 as confirmed by multiple biopsies to rule the lower grade lesions remain an issue. The tumour appears to the latter to the former occurs over a noma {419,1971,2813}. The epithelium is tive atypia of the nasopharyngeal epithe usually slightly thickened, and consists lium. Precursor lesions of cells with variable loss of polarity, There are only limited data on the natural In biopsies of nasopharyngeal carcino nuclear enlargement, nuclear crowding history of untreated pure nasopharyn geal carcinoma in-situ (or dysplasia). Histogenesis Nasopharyngeal carcinoma arises from the surface or crypt epithelium of the nasopharyngeal mucosa. In some cases, the tumour appears to arise from the basal layers of the stratified squamous epithelium, a finding further supported by the strong immunoreactivity for p63 in both the tumour and normal basal cells. The invasive carcinoma is accom multiple genetic alterations and Epstein panied by an abnormal surface epithelium comprising similar cells. Epidemiological studies strongly and thus contribute to the transformation of 3p21. Widespread hypermethylation of countries {382,1089,1223,1565,1567, and 20q were frequently detected CpG islands over the genome imply a 2365,2366}. Both the carcinoma cells and normal basal cells are immunoreactive sor gene on 9p21 by homozygous dele for p63. In a population-based acid alanine to valine, and it occurs adja nect phenotypes with genotypes. Significant improvements in treat showed that a 5-year disease-specific prognosis . Actuarial titers correlate significantly with survival disease-specific survival for different stages of nasopharyngeal carcinoma (Source of data: Hong {362,1547}. Eveson carcinomas Nasopharyngeal papillary sulated and infiltrate into the surrounding quency, adenoid cystic carcinoma, adenocarcinoma stroma. Carcinomas at this site frequently A low-grade adenocarcinoma character present; intraluminal and intracytoplas present at an advanced stage and often ized by an exophytic growth comprising mic mucicarmine staining may be focally with invasion of the base of the skull, papillary fronds and glandular structures. Immunohistochemical staining intracranial extension and involvement of shows positive reactivity for epithelial the cranial nerves. The microscopic features are similar Gender distribution is nearly equal A case has been reported in a patient to those of adenoid cystic carcinoma {1902,2672,2770}. Nasal obstruction is the main presenting Other rare salivary gland-type carcino symptom. The diagnosis can be readily Salivary gland-type carcinomas mas of the nasopharynx include epithe confirmed by endoscopic biopsy. Men are affected nearly three cell carcinoma and polymorphous the tumours are soft or gritty and exo times more frequently than women low-grade adenocarcinoma {1469,2763}. Tumour spread and staging the tumours usually remain confined within the nasopharynx except one reported case with extensive local inva sion . Histopathology Nasopharyngeal papillary adenocarcino ma arises from the surface epithelium . The lining columnar or pseudos tratified cells have bland, round to oval nuclei and tiny nucleoli. Psammoma bodies may be found in lined by columnar to spindly cells with bland-looking nuclei. Buchino Hairy polyp Prognosis and predictive factors section on sinonasal papillomas). A presumed developmental anomaly that clinically manifests as a polyp covered Schneiderian-type papilloma Prognosis and predictive factors by skin with hair and sebaceous glands. Local recurrences Synonyms A benign tumour that arises from the sur are not uncommon. Synonyms Fungiform papilloma, inverted papilloma, Squamous papillomas are uncommon in Localization transitional papilloma, nasopharyngeal the nasopharynx, and they are morpho the lateral wall of the nasopharynx, the papilloma. See chapter on Tumours of the soft palate, and the tonsils are classic Epidemiology hypopharynx, larynx and trachea. They Schneiderian-type papillomas of the also have been infrequently reported in nasopharynx are distinctly uncommon. No cases have They occur in older individuals (mean 62 Ectopic pituitary adenoma been reported in the sinonasal tract. Definition Clinical features A benign pituitary gland neoplasm the usual clinical presentation is a Etiology occurring separately from, and without pedunculated mass in the oropharynx or Anatomically, the posterior choanae rep involvement of the sella turcica. In the middle ear, the hairy polyps dermally-derived (Schneiderian mem cause recurrent otitis media that is not brane) and endodermally-derived respi responsive to the usual treatment. There ratory mucosa that, respectively, line the are individual reports of associated cleft sinonasal tract and nasopharynx. It is palate or multiple congenital anomalies, thought that aberrant embryologic dis including the Dandy-Walker malforma placement of normal Schneiderian tion . Histopathology the surface of the polyp is composed of Clinical features skin with a delicate hyperkeratotic layer Most do not exceed two cm in greatest and pilosebaceous units. They are often incidental find formed by fibroadipose tissue often with ings or, at most, result in nasal airway foci of cartilage, muscle and bone. The more common polyps are distinguished from teratomas Schneiderian papilloma of the sinonasal by a lack of endodermal components. Ectopic pitu congenital anomalies of the first itary adenoma of the nasopharynx appearing as a branchial cleft or choristomas . Histopathology submucosal and unencapsulated cellular tumour; They are similar to those occurring in the the nasopharyngeal surface epithelium is intact nasal cavity and paranasal sinuses (see and seen on top. Macroscopy Grossly, it is a polypoid and pedunculat ed mass ranging in size from 0. It is usually solitary; rare exam ples may occur synchronously in sepa A B rate sites . Histopathology Ectopic pituitary adenomas are submu cosal and unencapsulated cellular tumours with solid, organoid and trabec ular growth patterns; tumour nests are separated by fibrovascular stroma. The neoplastic cells have round to oval nuclei with dispersed nuclear chromatin, incon spicuous to small nucleoli, and granular C D cytoplasm that can be eosinophilic. Extracellular stro Scattered mitotic figures are seen in a tumour that otherwise shows uniform neoplastic cells with minimal mal hyalinization may be prominent. Extrasellar pituitary adenoma; extrasellar Localization adenohypophysial tissue; extracranial In the upper aerodigestive tract, ectopic Immunoprofile pituitary adenoma; sphenoidal pituitary pituitary adenoma most commonly Ectopic pituitary adenomas show strong adenoma; adenomatous pharyngeal occurs in the sphenoid bone and sinus cytoplasmic immunoreactivity for cytoker pituitary. Tumours may demonstrate and median age at presentation of 49 itary adenomas is primarily related to its immunoreactivity with only a single pitu years and 58 years respectively {1425, space occupying effects, and include air itary hormone (monohormonal pituitary 2752}. Females are affected more often way obstruction, chronic sinusitis, adenoma), multiple hormones (plurihor than men {1425,2752}. Clinical evi the etiology of ectopic pituitary adeno dence of hormonally active tumours can Electron microscopy mas is unknown. Extrasellar involvement be identified in over half of the cases Intracytoplasmic secretory granules of by a pituitary adenoma can result from and include Cushing disease varying numbers can be identified. However, com nation of Rathkes pouch (infrasellar) or tionship to the sella turcica . Of plete surgical resection may not be pos anterior pituitary cells attached to the note is the fact that the extent of tumour sible for larger, invasive tumours. When supradiagphragmatic portion of the pitu and erosion of bone do not completely resection is incomplete or cannot be itary stalk. This discussion will be limited correlate with severity of clinical signs accomplished due to size and extent of 100 Tumours of the nasopharynx A B. A the cellular tumour nodules communicate in the form of glandular structures with the surface epithelium. Dopa Almost all patients present with respirato the cellular nodules display a mixed pat mine agonist drugs. Bleeding has tern of reactivity for vimentin, cytokeratin have been effective in reducing the size rarely been reported. Clinical examina and actin and are generally non-reactive (not permanently) in prolactin-secreting tion reveals a midline pedunculated ery for S-100 protein and glial fibrillary acidic adenomas and the mitotic rate of other thematous polyp .
No clinical outcomes were reported medications used for depression depakote 500mg low price, and no evidence that these dose differences resulted in clinically meaningful improvement in results is presented medications during pregnancy generic 500 mg depakote mastercard. The authors acknowledged that proton radiotherapy in lung cancer raises many important issues among the most challenging of which is tumor motion during treatment resulting from the patients breathing medicine 8 pill generic depakote 500mg with amex. The most common grade 3 adverse effects related to proton therapy were dermatitis Page 28 of 263 and esophagitis symptoms for strep throat generic 500mg depakote amex, each experienced by 5 patients (11 treatment 02 bournemouth depakote 500mg online. Proton therapy to the gross tumor volume was given with weekly intravenous paclitaxel and carboplatin treatment refractory purchase depakote no prescription. This report focuses only on acute and subacute toxicity, because the follow-up duration is too short to evaluate tumor control and survival. The authors acknowledged several shortcomings of their study including the use of retrospective data for comparison, including substantial differences in pretreatment assessments (especially imaging) and treatment-planning capabilities over the periods of study and the heterogeneity of the patient populations. The proton therapy group was itself somewhat heterogeneous because of the inclusion of 25 patients with any stage (including recurrent) disease. Therefore differences in outcomes in this study are not clearly related to treatment modality. Non-hematologic and hematologic acute grade 3 toxicity (90 days) developed in 1 and 4 patients, respectively. Two of 16 patients assessable for late toxicity (90 days) developed a significant grade 3 non-hematologic late toxicity, whereas 1 patient developed a grade 3 hematologic late toxicity. Seven patients are currently alive without evidence of disease, and 7 other patients died from disease progression, including 6 with distant metastases as their first site of relapse and 1 with local progression as their first site of relapse. Larger prospective studies are needed to confirm these findings, define the critical dosimetric points that may be unique to proton therapy, and investigate the potential of proton therapy to facilitate radiation dose escalation and/or combined modality therapy. Patients were eligible for randomization only if both plans satisfied normal tissue constraints at the same radiation dose. The conclusion was that proton treatment did not improve dose-volume indices for lung but did for heart. They found that pain, as a major esophagitis-related symptom, increased more during therapy (p = 0. These results should be confirmed in a randomized study with comparable tumor burden among therapies. Considered together, these early reports of proton beam radiation for lung cancer are mostly single institution retrospective studies which do not demonstrate clearly superior outcomes compared to customary photon radiation techniques. For the cancers in group 2 it is essential to collect further data, especially to understand how the effectiveness of proton therapy compares to other radiation therapy modalities. There is a need for more well-designed registries and studies with sizable comparator cohorts to help accelerate data collection. Proton beam therapy for primary treatment of these cancers, including locally-advanced lung cancer, should only be performed within the context of a prospective clinical trial or registry. This is consistent with the investigational and unproven nature of Proton Beam Radiation Therapy for treatment of lung cancer. Until such data is available and until there is clear data documenting the clinical outcomes of proton beam therapy in the treatment of lung cancer, proton beam therapy remains unproven. Ablative techniques (Radiofrequency, Cryosurgery, Alcohol injection, Microwave) Several ablative techniques have been used both in the operable and definitive setting. For select lesions, generally under 3 cm in size that are well localized, definitive treatment may be considered. Contraindications to ablation include lack of anatomic accessibility, size, number, and location near abdominal organs, major ducts, and blood vessels. A complication reported with ablation is the development of tumor rupture with lesions located on the hepatic capsule or tumor seeding along the track with subcapsular and poorly differentiated lesions. Local control rates in the range of 90% at two years have been reported for ablative techniques. Indications for these procedures include multiple tumors, generally 4 or more in number, lesions greater than 3 to 5 cm, lesions without vascular invasion or extra-hepatic spread. Absolute contraindications include decompensated cirrhosis, jaundice, clinical encephalopathy, refractory ascites, hepatorenal syndrome, extensive tumor replacement of both lobes, portal vein occlusion or severely reduced flow, hepatofugal flow and renal insufficiency. Relative contraindications include tumor size greater than 10 cm, severe cardiovascular or pulmonary disease, varices at high risk of bleeding or bile duct occlusion. In addition to the contraindications listed above, all arterial therapies must take into account their effect on liver function as embolic-, chemo-, or radiation-liver disease or dysfunction can result in severe morbidity or death. Great care must be given in considering the individuals liver function, Hepatitis B carrier status, prior transarterial or other treatments, portal vein thrombosis, and Childs-Pugh score. A dose volume constraint to be considered is for the mean liver dose (liver minus gross tumor volume) to be less or equal to 28 Gy in 2 Gy fractions. The University of Michigan has demonstrated that tumoricidal doses from 40 Gy to 90 Gy delivered in 1. Sufficient hepatic reserve as evidenced by a Childs-Pugh A score is extremely important as safety data are considered limited in Childs Pugh B or those with poor liver reserve. Some controversy has existed over the Page 32 of 263 size of eligible lesions with initial restriction to lesions of up to 5 cm now being expanded to larger lesions. Current optimal dose recommendations are 50 Gy in 5 treatment fractions with a mean liver dose of 13. The unique dosimetric advantages of heavy charged particle radiation (Bragg Peak) offer significant potential advantages in sparing hepatic parenchyma compared to traditional photon techniques. This theoretical advantage is still the object of on-going studies in this country. A consultation note from Interventional Radiology documenting the contraindications as listed above to the use of ablative or transarterial techniques and 2. Documentation of tumor size not exceeding 16 cm in nominal diameter with the ability to maintain a normal function liver volume of 700 cc with proton treatment and 6. The ability to deliver a full hypofractionated proton treatment regimen of not less than 50 GyE in 22 fractions. The authors conclude that the initial results may serve in hypothesis formation for further investigation. There were no significant differences between the groups with each group receiving 70 Gy. On bivariable analysis, increased mean oral cavity dose was associated with a higher rate of G-tube placement; no patient required a G-tube if the mean oral cavity dose was < 26 Gy whereas all patients with a mean dose of > 41. In this analysis, 43 cohorts were identified; 30 treated with photons (1186 patients) and 13 with charged particles (286 patients). In an analysis of toxicity, charged particle therapy was found to be significantly associated with more neurological toxic effects (p = 0. The authors indicate that this could be related to reporting bias (significantly higher proportion of charged particle therapy studies reported toxic effects (p = 0. The authors state Significant proportions of patients in both groups still experienced moderate to severe symptoms during the chronic phase. Acute side effects included grade 3 dermatitis, mucositis, and dysphagia which occurred in 23, 29 and 12 patients respectively. Sixteen patients (32%) required evaluation in an emergency room during treatment with 10 subsequently requiring hospitalization primarily due to dehydration and pain from mucositis. The authors conclude that our findings demonstrate the feasibility and proof of principle of advanced proton therapy techniques delivering simultaneous integrated boost plansthus laying the ground work for a direct head-to-head comparison study. It was noted that patients receiving a G-tube during radiotherapy had significantly longer history of smoking, greater comorbidity, more advanced disease, greater need for bilateral treatment, higher use of induction chemotherapy and concurrent chemotherapy, and a longer duration of treatment. With regards to toxicity, there were no differences in acute toxicity by technique. Sites of treatment included the larynx (1), nasopharynx (5), paranasal sinus (2) and oropharynx (1). At a median follow up of 27 months, four patients (44%) achieved a complete response, four achieved a partial response without disease progression and one developed local progression. With respect to toxicity, four patients experienced grade 3 acute toxicities and one developed a grade 4 toxicity (blindness in the treated eye). This heterogeneous group of patients included 19 receiving treatment at initial diagnosis and seven receiving treatment at recurrence (six of whom had prior radiation and three of whom had pulmonary metastases). Twenty were treated after surgery with 18 of these exhibiting positive margins or gross residual disease. Longer follow-up is needed to gauge the durability of disease control and to monitor for late toxicities of therapy. Sites of treatment included lacrimal gland or sac (5), paranasal sinus (4), parotid gland (4), submandibular gland (2) and buccal mucosa (1). Median dose delivered was 60 Gy with 12 patients receiving concurrent chemotherapy. Four patients developed acute grade 3 toxicity and one patient experienced a grade 4 toxicity (blindness). An additional patient developed asymptomatic frontal lobe necrosis 18 months after treatment completion with near resolution at 24 months. The authors conclude that Page 38 of 263 Intensity-modulated proton therapy demonstrated comparable efficacy and safety when compared to other radiation modalities including other proton therapy delivery techniques. One additional patient refused radiation and chemotherapy after surgery but received stereotactic radiosurgery at the time of recurrence. Patients had stage T1N0 (1), T2N0 (6), T3N0 (1) or T4N0 (3), all without metastases. The authors conclude that globe-sparing surgery followed by adjuvant radiotherapy or concurrent chemoradiotherapy is associated with acceptable short-term locoregional control Holliday et al. Primary sites included the lacrimal gland (7), lacrimal sac/nasolacrimal duct (10) or eyelid (3). Seven patients experienced acute grade 3 while 9 patients developed chronic grade 3 ocular or eyelid function toxicity. Bivariate analysis revealed that a dose of 36 Gy or less to the ipsilateral cornea was associated with grade 3 chronic ocular toxicity (p = 0. The authors conclude that these findings suggest that adjuvant proton therapy can be delivered successfully after orbit-sparing surgery for epithelial tumors of the orbit and ocular adnexa. The authors conclude Reirradiation with proton therapy, with or without chemotherapy, provided reasonable locoregional disease control, toxicity profiles, and survival outcomes for an advanced-stage and heavily pretreated population. Additional data are needed to identify which patients are most likely to benefit from aggressive efforts to achieve local disease control and to evaluate the potential benefit of proton therapy relative to other modalities of reirradiation. Page 40 of 263 Lee et al. All plans were calculated to 55 Gy in 25 fractions with equivalent constraints and normalized to prescription dose. Protons also increased generalized equivalent uniform dose to duodenum and stomach, however these differences were small (< 5% and 10%, respectively; p < 0. Doses to other organs at risk were within institutional constraints and placed no obvious limitations on treatment planning. The authors concluded that protons are able to reduce the treated volume receiving low-intermediate doses, however the clinical significance of this remains to be determined. No patient demonstrated any grade 3 toxicity during treatment or during follow up. Chemotherapy was well-tolerated with a median of 99% of the prescribed doses delivered. Median follow up was 14 months for all patients and 23 months for surviving patients. No patient experienced a grade 3 or greater toxicity during treatment or follow up. Grade 2 toxicity was limited to a single patient Page 41 of 263 experiencing grade 2 fatigue. Of the remaining 50 patients, only 78% had surgery, with 16% found to be unresectable, 4% diagnosed with metastases prior to surgery, and 2% diagnosed with cholangiocarcinoma instead of pancreatic cancer. Six of 37 eligible resected patients (16%) experienced locoregional recurrence, while 73% developed distant metastases. The authors concluded that short-course proton-based chemoradiation is well tolerated and is associated with favorable local control in resectable pancreatic cancer (although 16% local failure after surgery and radiation, particularly with such limited follow up and early deaths, is not particularly favorable). Advanced immobilization techniques, such as the use of breath hold gating or targeting with implanted fiducial markers, were not used in this series, and the dose of 67. However, there was no statistical significance between the two groups regarding the median time to progression (15. This especially pertains to targets in the thorax and upper abdomen, including the pancreas, which move as a result of diaphragmatic excursion (Mori and Chen 2008; Mori, Wolfgang, and Lu et al. This could result in unanticipated overdose of normal tissues or under dose of target volumes. Therefore, direct comparative studies will be helpful to determine the relative safety and efficacy of protons relative to customary photon radiation. In addition, there are concerns about proton beam dose distributions in the setting of organ and respiratory motion and tissue differences and interfaces, as are seen in this location. Until such data is published and until there is clear data documenting the clinical outcomes of proton beam therapy in the treatment of cancer of the pancreas, proton beam therapy remains unproven. Seminoma the risks of radiation-induced second malignancy in seminoma are well documented. However, it must be recognized that use of anterior/posterior fields whether 2D or 3D are the very technique which has been the subject of these reports. They found a 19% increase in secondary primary malignancies in seminoma patients exposed to radiation therapy as compared to the general population including pancreas, non-bladder urothelial, bladder, thyroid, and others. An accompanying editorial in the journal noted an increased incidence of seminoma during the last 4 decades with improved survival, which makes the issue of radiation-induced malignancies of increasing concern. They identified risks of lung, bladder, pancreas, stomach, and other organs, noting that secondary primary cancers are a leading cause of death in men with a history of testicular cancer.
A chopulmonary aspergillosis without maintenance oral corticoste prospective observational study of candidemia: epidemiology treatment multiple sclerosis purchase discount depakote online, ther roids: a fteen-year follow-up treatment 32 buy depakote cheap. Nosocomial bloodstream infections in us hospitals: bronchopulmonary aspergillosis: a retrospective study of 35 cases medicine 8 pill generic 250 mg depakote overnight delivery. Therapeutic approaches in allergic bronchopulmonary aspergillosis with recombinant anti-ige patients with candidemia: evaluation in a multicenter treatment diffusion buy depakote 250mg cheap, prospective medicine shoppe discount depakote uk, antibody medicine 95a pill purchase depakote no prescription. Otani Y, Yoshida I, Ohki S, Kano M, Kawashima O, Suzuki M, Sato Y, other forms of invasive candidiasis. Cremaschi P, Nascimbene C, Vitulo P, Catanese C, Rota L, Barazzoni fections in neutropenic patients. Luzzati R, Amaltano G, Lazzarini L, Soldani F, Bellino S, Solbiati M, a successful treatment in 209 cases of relapse hemoptysis. Babatasi G, Massetti M, Chapelier A, Fadel E, Macchiarini P, Khayat of vascular catheters. Pneumocystis carinii pneumonia during Germany: consensus formed by a panel of interdisciplinary investi maintenance anti-tumor necrosis factor-alpha therapy with inix gators. Successful Should all patients with candidaemia have an ophthalmic examina intermittent chemoprophylaxis for Pneumocystis carinii pneumoni tion to rule out ocular candidiasis Empirical marrow transplantation is inferior to other regimens and is associ uconazole versus placebo for intensive care unit patients: a ran ated with decreased survival and an increased risk of other in domized trial. Use of Candida pneumonia: experience at a large cancer center and review a cyclophosphamide-induction methotrexate-maintenance regimen of the literature. National Institutes of Health-University of California expert panel for patients with hematologic malignancy who have zygomycosis. Posaconazole: a potent, extended-spectrum triazole anti therapy for pneumocystis pneumonia in the acquired immunode fungal for the treatment of serious fungal infections. A controlled trial of Posaconazole is effective as salvage therapy in zygomycosis: a retro early adjunctive treatment with corticosteroids for Pneumocystis carinii spective summary of 91 cases. Epidemiology, clinical manifestations, and V, Wagels T, Flepp M, Rickenbach M, Furrer H. Godeau B, Coutant-Perronne V, Le Thi Huong D, Guillevin L, center study from Italy and review of the literature. Immunotherapy for invasive fungal infections: from bench tissue disease: report of 34 cases. Gregory Stafel frst authored this short introduction to otolaryngology for medical students at the University of Texas School for the Health 1 Sciences in San Antonio in 1996. Written in conversational style, peppered with hints for learning (such as read an hour a day), and short enough to digest in one or two evenings, the book was a hit with medical students. We are grateful to the many authors and reviewers who have contributed over the years to the success of this publication. We anticipate that it will whet your appetite for further learning in the disci pline that we love and have found most intriguing. It should start your journey into otolaryngology, the feld of head and neck surgery. Sometimes individuals have trouble transitioning from being second-year medical students, where they are truly students, to becoming healthcare professionals. This metamorphosis over the third and fourth years of med ical school involves learning how to carry yourself and act as a healthcare professional. To meet this frst goal and become a good clinician, it is helpful for stu dents to be carefully observant of their professors in important but unno ticed aspects, such as their demeanor, comments, and interaction with house staf and patients. The process starts with the students appearance (clothing and grooming), punctuality, composure, acceptance of responsibility, and interactions with patients and other healthcare team members. However, medical students frequently have extra time to spend with their patients, talking to the patients about their past medical problems, family, and social history as they pertain to their disease process. This type of relationship establishes the medical student as an important part of the healthcare team, benefcial to the overall care provided to the patient. For the medical student, it also establishes long-term behaviors that translate into the development of an excellent future physician. During the third year, there may be conficting responsibilities, such as being at a lec ture while needing to draw a patients blood. If it is an important blood test and you cannot get someone to do it for you, you may need to miss the lecture. Tese situations dont actually come up that ofen, and if patient care is the main goal, over the long run, most people will respect these decisions. You should read textbooks because they cover the basics, and 90 percent of people do not know what is in them. It does not matter which textbook you read, because if the information is important, it will come up again in later reading. You are ready to read, and recall from your notes that your patient has hypertension, chronic obstructive pulmonary disease, diabetes, and a pleomorphic adenoma. Tere is no way you can read about all that tonight, and you have to get up at 5:00 a. So you go to bed, and the next morning you do not really know why we even treat asymptomatic hypertension in the frst place. Remember Darwins theory of medical education: It cannot be that rare if you are seeing it. You will be very compassionate to all your patients and coworkers, and you will always be willing and ready to learn. However, there is one important caveat that is ofen not addressed in medical educa tion: It is as much your responsibility to know your limitations as it is to know about treating patients. If you are trying hard, reading an hour every day, and truly interested, then if you are asked a question to which you do not know the answer, it is perfectly legitimate, and indeed expected, that you simply answer, I dont know. If you use the information you already have, you will ofen do surprisingly well if you guess at an answer. But if your answer is only a guess, qualify it by pointing out that you do not specifcally know the answer. Although you may not know that much yet in your clinical career, you have one secret weapon as a student: enthusiasm. Residents are ofen tired and grouchy, as you probably have noticed, but having an enthusiastic stu dent around makes a diference. Since the great majority of you will not become otolaryngologists, it becomes much more important for you to understand how to recognize potentially dangerous problems that should be referred to an otolaryngologist, as well as how to manage uncompli 6 cated problems that can be taken care of at the primary care level. Your highest professional priority throughout your third year and the rest of your career should be. One way to learn as much as possible, without feeling overwhelmed, during the third year is to . When faced with two conficting responsibilities, should always be your highest priority. The key to a happy career in medicine is to make your highest professional priority. In all countries of the world, a common vein through medicine is to keep as the frst priority. The head and neck exam involves inspection (and palpation if practical) of all skin and mucosal surfaces of the head and neck. Otolaryngologists utilize special equipment to better assess the ears, nose, and throat. A bin ocular microscope provides an enlarged, three-dimensional image, giving the physician a superior view of the ear canal and tympanic membrane. Fiberoptic instruments provide a similar ability to examine these regions, but with superior optics. The Ear Assess the external auricle for congenital deformities, such as microtia, promin auris, or preauricular pits. The external auditory canal should be examined by otoscopy afer being thoroughly cleaned if it is blocked by cerumen. The canal should be assessed for swelling, redness (erythema), narrowing (stenosis), discharge (otorrhea), and masses. Changes in the appearance of the eardrum may indicate pathology in the 10 middle ear, mastoid, or eustachian tube. White patches, called tympano sclerosis, are ofen clearly visible and provide evidence of prior signifcant infection. An erythematous, bulging, opacifed tympanic membrane indi cates acute bacterial otitis media. Healed perforations are ofen more trans parent than the surrounding drum and may be mistaken for actual holes. Pneumatic otoscopy should be performed to observe the mobility of the tympanic membrane with gentle insufation of air. Eustachian tube func tion may be assessed by watching the eardrum as the patient executes a gentle Valsalva. Tuning forks can be used to grossly assess hearing and to diferentiate between conductive and sensorineural hearing loss. A tuning fork placed in the center of the skull (Weber test) will normally be perceived in the mid line. The sound will lateralize and be perceived as louder on the afected side in cases of conductive hearing loss. If a sensorineural loss exists, the sound will be perceived in the better or normal hearing ear. The tuning fork is then placed just outside the external auditory canal for the Rinnes test of air conduction hearing. Placing the base of the tuning fork over the mastoid process allows bone conduction hearing to be assessed. In conduc tive hearing loss, the tuning fork is heard louder behind the ear (bone con duction is better than air conduction in conductive hearing losses). This is indicated in any patient with chronic hearing loss, or with acute loss that cannot be explained by canal occlusion or middle ear infection. Topical vasoconstriction with oxymetazoline permits a more thorough examination and allows for assessment of turbinate response to deconges tion. Nasal patency may be compromised by swollen boggy turbinates, septal deviation, nasal polyps, or masses/tumors. The remainder of the nasal cavity can be more carefully examined by performing fexible fberoptic or rigid nasal endoscopy. This allows a more thorough evalua tion of the nasal cavity and mucosa for abnormalities, including obstruc tion, lesions, infammation, and purulent sinus drainage. The sense of smell is rarely tested due to the difculty in objectively quantifying 11 responses. However, ammonia fumes can be useful for distinguishing true anosmics from malingerers because ammonia will stimulate trigeminal endings, and thus produce a response in the absence of any olfaction. The Mouth An adequate light and tongue depressor are necessary for examining the mouth. The tongue depressor should be used to systematically inspect all mucosal surfaces, including the gingivobuccal sulci, the gums and alveo lar ridge, the hard palate, sof palate, tonsils, posterior oropharynx, buccal mucosa, dorsal and ventral tongue, lateral tongue, and the foor of mouth. The parotid duct orifce (Stensons duct) can be seen on the buccal mucosa, opposite the upper second molar. The submandibular and sublingual glands empty into the foor of the mouth via Whartons ducts. Complete exami nation of the mouth includes bimanual palpation of the tongue and the foor of the mouth to detect possible tumors or salivary stones. The Pharynx The posterior wall of the oropharynx can be easily visualized via the mouth by depressing the tongue. Inspection of the nasopharynx, hypo pharynx, and larynx requires an indirect mirror exam or use of a fexible fberoptic rhinolaryngoscope. All mucosal surfaces are evaluated, to include the eustachian tube openings, adenoid, posterior aspect of the sof palate, tongue base, posterior and lateral pharyngeal walls, vallecula, epi glottis, arytenoid cartilages, vocal folds (false and true), and pyriform sinuses. Vocal fold mobility should be assessed by asking the patient to alternately phonate and snif deeply. The Neck The normal neck is supple, with the laryngotracheal apparatus easily pal pable in the midline. A complete examination should include external observation for symmetry and thorough palpation of all tissue for possible masses. The exact position, size, and character of any mass should be care fully noted, along with its relationship to other structures in the neck (thy roid, great vessels, airway, etc.
Order generic depakote online. What are the warning signs of flu complications?.
References
- Kilgore SP, Ormsby AH, Gramlich TL, et al: The gastric cardia: Fact or fiction? Am J Gastroenterol 95:921, 2000.
- Montalescot G, Borentain M, Payot L, et al. Early vs late administration of glycoprotein IIb/IIIa inhibitors in primary percutaneous coronary intervention of acute ST-segment elevation myocardial infarction: a meta-analysis. JAMA 2004;292:362-366.
- GISSI-HF Investigators. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSIHF trial): a randomized, double blind, placebo controlled trial. Lancet. 2008;372:1223-1230.
- Hashimoto K, Mayahara H, Takashima A, et al. Palliative radiation therapy for hemorrhage of unresectable gastric cancer: a single institute experience. J Cancer Res Clin Oncol 2009;135(8):1117-1123.
- Schuffler MD, Baird HW, Fleming CR, et al. Intestinal pseudoobstruction as the presenting manifestation of small cell carcinoma of the lung: a paraneoplastic neuropathy of the gastrointestinal tract. Arch Intern Med 1983;98:129.
- Metzger AL, Bohan A, Goldberg LS, Bluestone R, Pearson CM. Polymyositis and dermatomyositis: combined methotrexate and corticosteroid therapy. Ann Intern Med. 1974;81(2):182-189.
- Cussen LJ: Dimensions of the normal ureter in infancy and childhood, Invest Urol 5(2):164n178, 1967.
- Thompson KD, Welkyj S, Massa MC: Antibacterial activity of lidocaine in combination with a bicarbonate buffer. J Dermatol Surg Oncol 19: 216-220, 1993.

